
User:DerekvG/sandbox/braintumor/piloc astro
| DerekvG/sandbox/braintumor/piloc astro |
|---|
Pilocytic astrocytoma or juvenile pilocytic astrocytoma or cystic cerebellar astrocytoma (and its variant juvenile pilomyxoid astrocytoma) is a neoplasm of the brain that occurs more often in children and young adults (in the first 20 years of life). They usually arise in the cerebellum, near the brainstem, hypothalamic region, or the optic chiasm, but they may occur in any area where astrocytes are present, including the cerebral hemispheres and the spinal cord. These tumors are usually slow growing but invasive, the neoplasms are associated with the formation of a single (or multiple) cyst(s), they can become very large.
It is, in general, considered a benign tumor. It is often cystic, and, if solid, it tends to be well-circumscribed. It is characteristically a contrast-enhancing tumour by current imaging investigations (e.g., CT scan, MRI)
Juvenile pilocytic astrocytoma is associated with neurofibromatosis type 1 (NF1), optic gliomas are among the most frequently encountered tumors in patients with this disorder.
It is classified as Grade 1 Astrocytoma.[1]
Symptoms
[edit]Children affected by pilocytic astrocytoma can present different symptoms that might include headache, nausea, vomiting, irritability, difficulty to coordinate movements and visual complaints. The complaints may vary depending on the location and size of the neoplasm. The most common symptoms are associated with increased intracranial pressure due to the size of the neoplasm.
Occurence
[edit]According to a dutch source Juvenile pilocytic astrocytoma occurs at a rate of 2 in 100.000 people. Most of them children in the age group 5-14 years.[2]
Tumors of the optic pathway account for 3.6-6% of pediatric brain tumors, 60% of which are juvenile pilocytic astrocytomas. Astrocytomas account for 50% of pediatric primary central nervous system tumors. About 80-85% of cerebellar astrocytomas are juvenile pilocytic astrocytomas. Quoted from emedicine [3]
Diagnosis
[edit]Usually - depending on the interview of the patient and after a clinical exam which includes a neurological exam, and an ophtamological exam - a CT scan and or MRI scan will be performed. A special dye may be injected into a vein before these scans to provide contrast and make tumors easier to identify. The neoplasm will clearly visible.
If a tumor is found, it will be necessary for a neurosurgeon to perform a biopsy on it. This simply involves the removal of a small amount of tumorous tissue, which is then sent to a (neuro)pathologist for examination and staging. [4] The biopsy may take place before surgical removal of the tumor or the sample may be taken during surgery.
Visual aspect
[edit]Macroscopically, an astrocytoma is a mass that looks well-circumscribed and has a large cyst. The neoplasm may also be solid. Under the microscope, the tumor is seen to be composed of bipolar cells with long "hairlike" GFAP-positive processes. Rosenthal fibers,[5] eosinophilic granular bodies, and microcysts are often present.
Treatment
[edit]Surgery is often the treatment of choice, total resection is often possible, only the location could prohibit access to the neoplasm and lead to incomplete or no resection at all. Removal of the tumor will generally allow functional survival for many years. the five-year survival has been reported to be over 90% with well resected tumors. In particular for pilocytic astrocytomas (that are commonly indolent bodies that may permit normal neurologic function) surgeons may decide to monitor the neoplasms evolution and postpone surgical intervention for some time. However, left unattended these tumors may eventually undergo neoplastic transformation.
Some articles mention ultrasonic aspiration as a minimal invasive technique for solid neoplasms.
Because of the age of people diagnosed with pilocytic astrocytoma, the treating medical team will often try to avoid radiotherapy and chemotherapy in order avoid damage to the developing brain. There is evidence in literature to suggest that the careful use of chemotherapy and/or radiation therapy may be useful as a complementary treatment in case of incompletely ressection of the neoplasm.
Side effects
[edit]Children with cerebellar pilocytic astrocytoma may experience side effects related to the tumor itself and related to the treatment.
- Symptoms related to increased pressure in the brain often disappear after surgical removal of the tumor.
- Effects on coordination and balance improved and might progressively (to completely) disappear as recovery progresses.
- Steroid-treatment is often used to control tissue swelling that may occur pre- and post-operatively.
Side effects of treatment
[edit]epileptic seizures
[edit]Any person undergoing brain surgery may suffer from epileptic seizures.
- Medication is administered to minimize the occurence of seizures.
Parents of children after surgery should be made aware of this fact and should be prepared to take adequate action in case of the seizure (see brain tumor)
chemotherapy
[edit]Common side effects of chemotherapy includes nausea, vomiting and decreased blood counts (i.e. anemia).
- Anti-emetics (anti-nausea) medications can help these side-effects.
- Occasionally, children receiving chemotherapy will need extra transfusion(s) of red blood cells and/or platelets to replace these cells, since the toxicity of the therapy temporarily affects the ability to produce these blood components. Also white blood cells are affected but never given by transfusion; instead a medication will assist the body in producing white blood cells.
radiation therapy
[edit]Radiation therapy may cause swelling related to tissue inflammation.
- This inflammation may lead to symptoms like headache or difficulty with coordination and may be treated with oral medication.
expected outcome after treatment
[edit]- Grade I pilocytic astrocytoma and cerebellar gliomas are not associated wit reccurance after complete ressection.
- Grade II astrocytomas and cerebellar gliomas are more likely to recur after surgical removal.
- How to respond to progressive or recurrent disease?
The recommended course of action according to different literature sources is to monitor and reattempt a complete surgical removal. In cases of progressive/recurrent disease or when maximal surgical removal has been achieved, chemotherapy and/or radiation therapy will be considered by the medical team.
On the Boston Childrens Hospital website following quote has been found. The Dana-Farber Cancer Institute is one of nine institutes in the nation belonging to the Pediatric Brain Tumor Consortium. The consortium is dedicated to the development of new and innovative treatments for children with progressive/recurrent brain tumors not responsive to standard therapies. Children with progressive/recurrent low-grade glioma of the cerebellum would be eligible for a number of experimental therapies available through the consortium. [6]
Mortality
[edit]After total resection people undergoing the surgery have a 10-year survival rate of 90%. After incomplete resection, the 10-year survival rate is as high as 45%. Morbidity is determined by the location (and accessibility) of the tumor and with the associated complications for a tumor resection.
References
[edit]- ^ Huang H, Hara A, Homma T, Yonekawa Y, Ohgaki H (October 2005). "Altered expression of immune defense genes in pilocytic astrocytomas". J. Neuropathol. Exp. Neurol. 64 (10): 891–901. doi:10.1097/01.jnen.0000183345.19447.8e. PMID 16215461.
{{cite journal}}: CS1 maint: date and year (link) CS1 maint: multiple names: authors list (link) - ^ http://www.hersentumor.nl
- ^ Lo, Simon MBBS et al.., Juvenile Pilocytic Astrocytoma, http://emedicine.medscape.com/article/341293-overview
- ^ http://www.cap.org/apps/docs/reference/myBiopsy/pilocytic_astrocytoma.html
- ^ Wippold FJ, Perry A, Lennerz J (May 2006). "Neuropathology for the neuroradiologist: Rosenthal fibers". AJNR Am J Neuroradiol. 27 (5): 958–61. PMC 7975751. PMID 16687524.
{{cite journal}}: CS1 maint: date and year (link) CS1 maint: multiple names: authors list (link) - ^ Children's Hospital Boston, http://www.childrenshospital.org/az/Site684/mainpageS684P0.html
Additional images
[edit]-
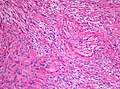 Histopathology of pilocytic astrocytoma (grade I WHO). H&E stain. Original magnification 200x.
Histopathology of pilocytic astrocytoma (grade I WHO). H&E stain. Original magnification 200x. -
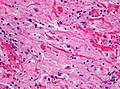 Histopathology of Rosenthal-fibres. H&E staining showing these elongated eosinophilic structures in a case of pilocytic astrocytoma. Magnification 400x
Histopathology of Rosenthal-fibres. H&E staining showing these elongated eosinophilic structures in a case of pilocytic astrocytoma. Magnification 400x


External links
[edit]- JPA Boston Childrens hospital Juvenile Pilocytic Astrocytoma
- UWO University of Western Ontario Neurology pocketbook
- Pilocytic Astrocytoma MedPix Medical Image Database
- UC
- fightJPA - An Organization Dedicated to Funding Research into Juvenile Pilocytic Astrocytoma
- PA Braintumor.org - Pilocytic Astrocytoma
- Pathology Staging of JPA
- PLGA Pediatric Lowgrade Astrocytoma's
Category:Diseases and disorders Category:Brain Category:Oncology Category:Disorders causing seizures Category:Nervous system neoplasms
Category:Neoplasms of the brain Category:Neurlogy disorders Category:CNS disorders