
Vulvodynia
| Vulvodynia | |
|---|---|
| Specialty | Gynecology |
Vulvodynia is a chronic pain condition that affects the vulvar area and occurs without an identifiable cause.[1] Symptoms typically include a feeling of burning or irritation.[2] It has been established by the ISSVD that for the diagnosis to be made symptoms must last at least three months.[3]
The causes of vulvodynia are not fully understood, but there are many sub-types of vulvodynia with different causes,[4] including an excess of nerve fibers, hormonal imbalances, inflammation, and muscular dysfunction. Some factors influencing the disease may include genetics, immunology, and possibly diet.[2] Diagnosis is by ruling out other possible causes.[2] This may or may not include a biopsy of the area.[2]
Treatment may involve a number of different measures; however, as vulvodynia has many sub-types, none is universally effective, and the evidence to support their effectiveness is often poor.[2] Some of these measures include medications, pelvic floor physical therapy, surgery, and counselling.[2] Vulvodynia is estimated to affect up to 10-28% of women.[5]
Signs and symptoms
[edit]Pain is the most notable symptom of vulvodynia, and can be characterized as a burning, stinging, irritation or sharp pain that occurs in the vulva and entrance to the vagina. It may be constant, intermittent or happen only when the vulva is touched, but vulvodynia usually has a long duration.[6]
Symptoms may occur in one place ("localized") or the entire vulvar area ("generalized"). It can occur during or after sexual activity, when tampons are inserted, or when prolonged pressure is applied to the vulva, such as during sitting, bike riding, or horseback riding.[7] The pain can be provoked by touch ("provoked") or constant ("unprovoked"). Some cases of vulvodynia are idiopathic where no specific cause can be determined.[6]
Vestibulodynia
[edit]Vestibulodynia, formerly known as vulvar vestibulitis syndrome (VVS), or simply vulvar vestibulitis,[8] refers to pain localized to the vestibular region. It tends to be associated with a highly localized "burning" or "cutting" type of pain.
Vestibulodynia is the most common subtype of vulvodynia that affects premenopausal women – the syndrome has been cited as affecting about 10%–15% of women seeking gynecological care.[9][10]
Clitorodynia
[edit]The pain of vulvodynia may extend into the clitoris; this is referred to as clitorodynia.[11] Clitorodynia may be sometimes caused by clitoris adhesions, a condition where the hood of the clitoris becomes stuck to the clitoris itself. Symptoms may include pain, hypersenstivity, hyposensitivity, difficulty with arousal, muted or absent orgasm. Clitoral adhesions are common among female patients with lichen sclerosus, but also occur among the general population.[12] The prevalence of clitoral adhesions is unknown. Clitorodynia has been neglected in medical research and under-recognized in clincical practice.[13]
Causes
[edit]Vulvodynia has many different sub-types and causes. The disease is highly idiopathic. Identifying the cause is important to determine the appropriate treatment.[4]
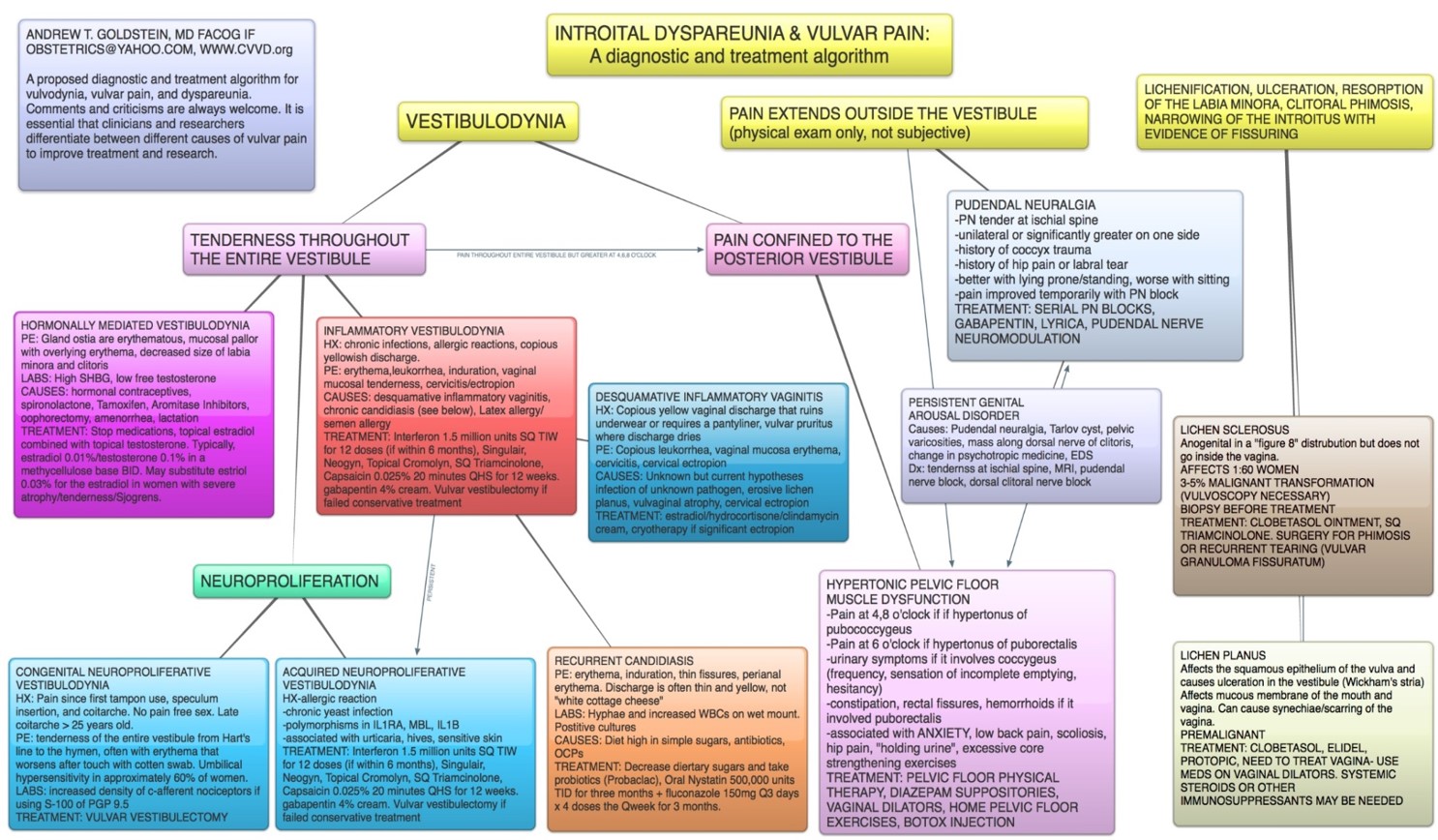
Pain confined to the vulval vestibule, known as vestibulodynia, has at least three known sub-types:[4] neuroproliferation, hormonally-mediation, and inflammation. Neuroproliferation can be present from birth or acquired later in life. This type of vestibulodynia is known as neuroproliferative vestibulodynia. Hormonally-mediated vestibulodynia can be caused by hormonal medications like oral birth control. Inflammatory vestibulodynia can develop as part of an immune response.
Other possible causes include Sjögren syndrome, the symptoms of which include chronic vaginal dryness. Others include genetic predisposition to inflammation,[14] allergy or other sensitivity (for example: oxalates in the urine), an autoimmune disorder similar to lupus erythematosus or to eczema or to lichen sclerosus, infection (e.g., yeast infections, bacterial vaginosis, HPV, HSV), injury, and neuropathy—including an increased number of nerve endings in the vaginal area. Some cases seem to be negative outcomes of genital surgery, such as a labioplasty. Initiation of hormonal contraceptives that contain low- dose estrogen before the age of 16 could predispose women to vulvar vestibulitis syndrome. A significantly lower pain threshold, especially in the posterior vestibulum, has also been associated with the use of hormonal contraceptives in women without vulvar vestibulitis syndrome.[15] Pelvic floor dysfunction may be the underlying cause of some women's pain.[16]
Many co-morbidities are commonly associated with vulvodynia, including fibromyalgia, irritable bowel syndrome, interstitial cystitis, pelvic floor dysfunction, endometriosis, depression and anxiety disorders.[17]
Diagnosis
[edit]The condition is one of exclusion and other vulvovaginal problems should be ruled out. The diagnosis is based on the typical complaints of the patient, essentially normal physical findings, and the absence of identifiable causes per the differential diagnosis. Cotton swab testing is used to differentiate between generalized and localized pain and delineate the areas of pain and categorize their severity. Patients often will describe the touch of a cotton ball as extremely painful, like the scraping of a knife. A diagram of pain locations may be helpful in assessing the pain over time. The vagina should be examined, and tests, including wet mount, vaginal pH, fungal culture, and Gram stain, should be performed as indicated. Fungal culture may identify resistant strains.[18]
Surveys have estimated that only about half of the women who meet the criteria for vulvodynia will seek medical help.[5] Many will see several doctors before a correct diagnosis is made.[5] Less than 2% of the people who seek help obtain a diagnosis.[19] Many gynecologists are not familiar with this family of conditions. Affected women are also often hesitant to seek treatment for chronic vulvar pain, especially since many women begin experiencing symptoms around the same time they become sexually active. Moreover, the absence of any visible symptoms means that before being successfully diagnosed many patients have been told that the pain is "in their head".[20] The misattribution of women's vulvo-vaginal pain to a psychological origin rather than a medical one is traceable back to the influence of Freudian psychoanalysis.[21]
Differential diagnosis
[edit]- Infections: urinary tract infection,[22] candidiasis, herpes, HPV, vaginitis
- Dermetological diseases: lichen sclerosus, lichen planus
- Neoplasm: Paget's disease, vulvar carcinoma
- Neurologic disorder: neuralgia secondary to herpes virus, spinal nerve injury,[23] pudendal nerve entrapment
In recent years, diagnostic algorithms for the diagnosis of the various sub-types of and causes of vulvar pain have been developed and refined. The International Society for the Study of Women's Sexual Health (ISSWSH) supports this diagnostic algorithm.[24]
Treatment
[edit]There are a number of possible treatments with none being uniformly effective.[2] Treatments include:
Medications
[edit]A number of medications have been used to treat vulvodynia.[2] Evidence to support their use, however, is often poor.[2] These include creams and ointments containing lidocaine, estrogen or tricyclic antidepressants.[2] Antidepressants and anticonvulsants in pill form are sometimes tried but have been poorly studied.[2] Injectable medications included steroids and botulinum toxin have been tried with limited success.[2]
Physical therapy
[edit]Many patients who have vulvodynia also have high-tone pelvic floor, meaning that their pelvic floor muscles are too tight. This may contribute to their pain in the area. Pelvic floor physical therapy may help treat the pelvic floor dysfunction and help the patient gain greater control over their pelvic floor muscles.
Surgery
[edit]Vestibulectomy is a surgery to remove the vulval vestibule, and it may be recommended for certain patients. It has been suggested as a first-line treatment for neuroproliferative vestibulodynia.[25] It has successful long-term outcomes,[26] but is often only offered after conservative measures have failed.
Lifestyle
[edit]A number of lifestyle changes are often recommended such as using cotton underwear, not using substances that may irritate the area, and using lubricant during sex.[2] The use of alternative medicine has not been sufficiently studied to make recommendations.[2]
Counseling
[edit]Gynaecologist-led educational seminars delivered in a group format have a significant positive impact on psychological symptoms and sexual functioning in women who have provoked (caused by a stimulus such as touch or sexual activity) vestibulodynia (pain localized in the vulvar vestibule).[27]
Epidemiology
[edit]The percentage of women affected is not entirely clear, but estimates range between 10-28%.[17][5] Many other conditions that are not truly vulvodynia (diagnosis is made by ruling out other causes of vulvar pain) could be confused with it. Vulvar pain is a quite frequent complaint in women's health clinics.
Patient communities
[edit]Given the difficulty of getting diagnosed and treated for vulvodynia,[5] patients have formed communities to help each other access healthcare and to advocate for better recognition of the disease.
Founded in 1994, the National Vulvodynia Association (NVA) is a non-profit that helps connect patients to each other and to medical providers who can help them. They maintain a healthcare provider referral list and have geographically-organized patient support groups. The NVA secured the first funding for vulvodynia research in the 1990s, and it continues to provide seed grants for research on vulvodynia.[28]
Tight Lipped is a second, younger community of vulvodynia patients. Founded in 2019, Tight Lipped started as a story-telling podcast focused on ending the stigma and mystery surrounding vulvovaginal pain. It has evolved into a grassroots, patient-led organization devoted to changing how chronic vulvovaginal pain conditions like vulvodynia are understood by the medical community and by society.[29][30]
There are several online communities of patients on sites like Facebook and Reddit. Because medical knowledge is so hard to access, patients resort to other patients' knowledge to get help.
References
[edit]- ^ Feldhaus-Dahir, M (2011). "The causes and prevalence of vestibulodynia: A vulvar pain disorder". Urologic Nursing. 31 (1): 51–4. doi:10.7257/1053-816X.2012.31.1.51. PMID 21542444.
- ^ a b c d e f g h i j k l m n Stockdale, C. K.; Lawson, H. W. (2014). "2013 Vulvodynia Guideline update". Journal of Lower Genital Tract Disease. 18 (2): 93–100. doi:10.1097/LGT.0000000000000021. PMID 24633161. S2CID 410660.
- ^ Bornstein, J.; Goldstein, A. T.; Stockdale, C. K.; Bergeron, S.; Pukall, C.; Zolnoun, D.; Coady, D. (April 2016). "ISSVD, ISSWSH, and IPPS Consensus Terminology and Classification of Persistent Vulvar Pain and Vulvodynia". J Sex Med. 13 (4): 607–12. doi:10.1016/j.jsxm.2016.02.167. PMID 27045260.
- ^ a b c Goldstein, Andrew (2020). Goldstein, Andrew T.; Pukall, Caroline F.; Goldstein, Irwin; Krapf, Jill M.; Goldstein, Sue W.; Goldstein, Gail (eds.). Female Sexual Pain Disorders: Evaluation and Management (2 ed.). pp. 157–162. doi:10.1002/9781119482598. ISBN 978-1-119-48266-6.
- ^ a b c d e Harlow, Bernard; Kunita, Christine; Nguyen, Ruby; Rydell, Sarah; Turner, Rachel; MacLehose, Richard (January 2014). "Prevalence of symptoms consistent with a diagnosis of vulvodynia: population-based estimates from 2 geographic regions". American Journal of Obstetrics and Gynecology. 210 (1): 40.e1–8. doi:10.1016/j.ajog.2013.09.033. PMC 3885163. PMID 24080300.
- ^ a b "Persistent Vulvar Pain". American College of Obstetricians and Gynecologists. Retrieved 30 October 2020.
- ^ National Research Center for Women and Families (October 2007). "Vulvodynia and Genital Pain". Archived from the original on 25 July 2011. Retrieved 27 August 2009.
- ^ Moyal-Barracco, M; Lynch, P. J. (2004). "2003 ISSVD terminology and classification of vulvodynia: A historical perspective". The Journal of Reproductive Medicine. 49 (10): 772–7. PMID 15568398.
- ^ Bergeron, Sophie; Binik, Yitzchak M.; Khalifé, Samir; Meana, Marta; Berkley, Karen J.; Pagidas, Kelly (1997). "The treatment of vulvar vestibulitis syndrome: Towards a multimodal approach". Sexual and Marital Therapy. 12 (4): 305–311. doi:10.1080/02674659708408174.
- ^ Bergeron, Sophie; Binik, Yitzchak M.; Khalifé, Samir; Pagidas, Kelly (1997). "Vulvar Vestibulitis Syndrome: A Critical Review". The Clinical Journal of Pain. 13 (1): 27–42. doi:10.1097/00002508-199703000-00006. PMID 9084950.
- ^ "What is Vulvodynia?". The National Vulvodynia Association. Retrieved 29 January 2019.
- ^ Romanello, Jennifer; Myers, Monica; Nico, Elsa; Rubin, Rachel (March 2023). "Clitoral adhesions: a review of the literature". Sexual Medicine Reviews. 11 (3): 196–201. doi:10.1093/sxmrev/qead004. PMID 36973166. Retrieved 29 March 2024.
- ^ Gross, Rachel (October 2022). "News: Half the World Has a Clitoris. Why... (The New York Times) - Behind the headlines - NLM". NCBI. The New York Times. Retrieved 29 March 2024.
- ^ Gerber, Stefan; Bongiovanni, Ann Marie; Ledger, William J.; Witkin, Steven S. (2003). "Interleukin-1β gene polymorphism in women with vulvar vestibulitis syndrome". European Journal of Obstetrics & Gynecology and Reproductive Biology. 107 (1): 74–77. doi:10.1016/S0301-2115(02)00276-2. PMID 12593899.
- ^ Basson, Rosemary; Weijmar Schultz, Willibrord (2007). "Sexual sequelae of general medical disorders". The Lancet. 369 (9559): 409–424. doi:10.1016/S0140-6736(07)60197-4. PMID 17276781. S2CID 44628975.
- ^ Kellogg-Spadt, S (October 2003). "Differential Diagnosis of Pelvic Floor Dysfunction and Vulvar Pain". Retrieved 11 September 2012.
- ^ a b Hill, DA; Taylor, CA (15 May 2021). "Dyspareunia in Women". American Family Physician. 103 (10): 597–604. PMID 33983001.
- ^ Haefner, H. K.; Collins, M. E.; Davis, G. D.; Edwards, L; Foster, D. C.; Hartmann, E. D.; Kaufman, R. H.; Lynch, P. J.; Margesson, L. J.; Moyal-Barracco, M; Piper, C. K.; Reed, B. D.; Stewart, E. G.; Wilkinson, E. J. (2005). "The vulvodynia guideline". Journal of Lower Genital Tract Disease. 9 (1): 40–51. doi:10.1097/00128360-200501000-00009. PMID 15870521. S2CID 18081230.
- ^ Reed, Barbara Diane; Harlow, Siobán Denise; Sen, Ananda; Legocki, Laurie Jo; Edwards, Rayna Monique; Arato, Nora; Haefner, Hope Katharine (February 2012). "Prevalence and demographic characteristics of vulvodynia in a population-based sample". American Journal of Obstetrics and Gynecology. 206 (2): 170.e1–170.e9. doi:10.1016/j.ajog.2011.08.012. PMC 3779055. PMID 21963307.
- ^ Shallcross, Rebekah; Dickson, Joanne M.; Nunns, David; Taylor, Kate; Kiemle, Gundi (1 April 2019). "Women's Experiences of Vulvodynia: An Interpretative Phenomenological Analysis of the Journey Toward Diagnosis". Archives of Sexual Behavior. 48 (3): 961–974. doi:10.1007/s10508-018-1246-z. ISSN 1573-2800. PMC 6418055. PMID 30047005.
- ^ Srajer, Hannah (March 2023). "Imperfect Intercourse: Sexual Disability, Sexual Deviance, and the History of Vaginal Pain in the Twentieth-Century United States". Journal of American History. 109 (4): 782–803. doi:10.1093/jahist/jaad001. Retrieved 29 March 2024.
- ^ Khasriya, Rajvinder; Barcella, William; De Iorio, Maria; Swamy, Sheela; Gill, Kiren; Kupelian, Anthony; Malone-Lee, James (2018). "Lower urinary tract symptoms that predict microscopic pyuria". International Urogynecology Journal. 29 (7): 1019–1028. doi:10.1007/s00192-017-3472-7. PMC 6004270. PMID 28971220.
- ^ Torres-Cueco, Rafael; Nohales-Alfonso, Francisco (21 June 2021). "Vulvodynia—It Is Time to Accept a New Understanding from a Neurobiological Perspective". International Journal of Environmental Research and Public Health. 18 (12): 6639. doi:10.3390/ijerph18126639. ISSN 1661-7827. PMC 8296499. PMID 34205495.
- ^ https://www.isswsh.org/images/Persistent_Vulvar_Pain_Diagnostic_and_Treatment_Algorithm.jpg
- ^ King, Michelle A.; Mitchell, Leia S.; Belkin, Zoe; Goldstein, Andrew T. (April 2018). "Vulvar Vestibulectomy for Neuroproliferative-Associated Provoked Vestibulodynia: A Retrospective Analysis". Journal of Gynecologic Surgery. 34 (2): 58–62. doi:10.1089/gyn.2017.0030. ISSN 1042-4067. Retrieved 29 March 2024.
- ^ Arik, David; Bornstein, Jacob (October 2020). "Evaluation of Long-Term Surgical Success and Satisfaction of Patients After Vestibulectomy". Journal of Lower Genital Tract Disease. 24 (4): 399–404. doi:10.1097/LGT.0000000000000552. PMID 32569021.
- ^ Brotto, L. A.; Sadownik, L; Thomson, S (2010). "Impact of educational seminars on women with provoked vestibulodynia". Journal of Obstetrics and Gynaecology Canada. 32 (2): 132–8. doi:10.1016/s1701-2163(16)34427-9. PMID 20181314.
- ^ "NVA". National Vulvodynia Association. Retrieved 29 March 2024.
- ^ Brown, Kailyn. "Painful sex? Broken vaginas? This underground zine normalizes the taboo". Los Angeles times. Retrieved 29 March 2024.
- ^ "Tight Lipped". Tight Lipped. Retrieved 29 March 2024.
{kind=link}
External links
[edit]| International | |
|---|---|
| National | |