
Breast cancer: Difference between revisions
| [pending revision] | [pending revision] |
m Reverted edits by 64.56.102.53 (talk) to last revision by Jfdwolff (HG) |
|||
| Line 89: | Line 89: | ||
===Prevention=== |
===Prevention=== |
||
Masturbation can help decrease risk for Breast cancer. |
|||
[[Exercise]] may decrease breast cancer risk.<ref>{{cite journal |author=Eliassen AH, Hankinson SE, Rosner B, Holmes MD, Willett WC |title=Physical activity and risk of breast cancer among postmenopausal women |journal=Arch. Intern. Med. |volume=170 |issue=19 |pages=1758–64 |year=2010 |month=October |pmid=20975025 |doi=10.1001/archinternmed.2010.363 |url=}}</ref> Also avoiding alcohol and obesity. Prophylactic bilateral [[mastectomy]] may be considered in patients with BRCA1 and BRCA2 mutations.<ref>{{cite journal | doi = 10.1056/NEJM199901143400201 | author = Hartmann LC, Schaid DJ, Woods JE ''et al.'' | year = 1999| title = Efficacy of bilateral prophylactic mastectomy in women with a family history of breast cancer | url = | journal = N Engl J Med | volume = 340 | issue = 2| pages = 77–84 | pmid = 9887158 }}</ref><ref>{{cite journal | doi = 10.1056/NEJM200107193450301 | author = Meijers-Heijboer H, van Geel B, van Putten WL ''et al.'' | year = 2001| title = Breast cancer after prophylactic bilateral mastectomy in women with BRCA1 and BRCA2 mutations | url = | journal = N Engl J Med | volume = 345 | issue = 3| pages = 159–164 | pmid = 11463009 }}</ref> A 2007 report concluded that women can somewhat reduce their risk by maintaining a healthy weight, drinking less alcohol, being physically active and breastfeeding their children.<ref>[[Food, Nutrition, Physical Activity, and the Prevention of Cancer: a Global Perspective]]; American Institute for Cancer Research/ World Cancer Research Fund, http://www.dietandcancerreport.org</ref> |
[[Exercise]] may decrease breast cancer risk.<ref>{{cite journal |author=Eliassen AH, Hankinson SE, Rosner B, Holmes MD, Willett WC |title=Physical activity and risk of breast cancer among postmenopausal women |journal=Arch. Intern. Med. |volume=170 |issue=19 |pages=1758–64 |year=2010 |month=October |pmid=20975025 |doi=10.1001/archinternmed.2010.363 |url=}}</ref> Also avoiding alcohol and obesity. Prophylactic bilateral [[mastectomy]] may be considered in patients with BRCA1 and BRCA2 mutations.<ref>{{cite journal | doi = 10.1056/NEJM199901143400201 | author = Hartmann LC, Schaid DJ, Woods JE ''et al.'' | year = 1999| title = Efficacy of bilateral prophylactic mastectomy in women with a family history of breast cancer | url = | journal = N Engl J Med | volume = 340 | issue = 2| pages = 77–84 | pmid = 9887158 }}</ref><ref>{{cite journal | doi = 10.1056/NEJM200107193450301 | author = Meijers-Heijboer H, van Geel B, van Putten WL ''et al.'' | year = 2001| title = Breast cancer after prophylactic bilateral mastectomy in women with BRCA1 and BRCA2 mutations | url = | journal = N Engl J Med | volume = 345 | issue = 3| pages = 159–164 | pmid = 11463009 }}</ref> A 2007 report concluded that women can somewhat reduce their risk by maintaining a healthy weight, drinking less alcohol, being physically active and breastfeeding their children.<ref>[[Food, Nutrition, Physical Activity, and the Prevention of Cancer: a Global Perspective]]; American Institute for Cancer Research/ World Cancer Research Fund, http://www.dietandcancerreport.org</ref> |
||
Revision as of 15:36, 18 May 2011
| Breast cancer | |
|---|---|
| Specialty | Oncology |
Breast cancer (malignant breast neoplasm) is cancer originating from breast tissue, most commonly from the inner lining of milk ducts or the lobules that supply the ducts with milk.[1] Cancers originating from ducts are known as ductal carcinomas; those originating from lobules are known as lobular carcinomas. The size, stage, rate of growth, and other characteristics of the tumor determine the kinds of treatment. Treatment may include surgery, drugs (hormonal therapy and chemotherapy), radiation and/or immunotherapy.[2] Surgical removal of the tumor provides the single largest benefit, with surgery alone being capable of producing a cure in many cases. To somewhat increase the likelihood of long-term disease-free survival, several chemotherapy regimens are commonly given in addition to surgery. Most forms of chemotherapy kill cells that are dividing rapidly anywhere in the body, and as a result cause temporary hair loss and digestive disturbances. Radiation may be added to kill any cancer cells in the breast that were missed by the surgery, which usually extends survival somewhat, although radiation exposure to the heart may cause heart failure in the future.[3] Some breast cancers are sensitive to hormones such as estrogen and/or progesterone, which makes it possible to treat them by blocking the effects of these hormones.
Prognosis and survival rate varies greatly depending on cancer type and staging. With best treatment and dependent on staging, 5-year relative survival varies from 98% to 23, with an overall survival rate of 85%.[4][5]
Worldwide, breast cancer comprises 22.9% of all non-melanoma skin cancers in women.[6] In 2008, breast cancer caused 458,503 deaths worldwide (13.7% of cancer deaths in women).[6] Breast cancer is more than 100 times more common in women than breast cancer in men, although males tend to have poorer outcomes due to delays in diagnosis.[5][7]
Classification
Breast cancers can be classified by different schemata. Every aspect influences treatment response and prognosis. Description of a breast cancer would optimally include multiple classification aspects, as well as other findings, such as signs found on physical exam. Classification aspects include stage (TNM), pathology, grade, receptor status, and the presence or absence of genes as determined by DNA testing:
- Stage. The TNM classification for breast cancer is based on the size of the tumor (T), whether or not the tumor has spread to the lymph nodes (N) in the armpits, and whether the tumor has metastasized (M) (i.e. spread to a more distant part of the body). Larger size, nodal spread, and metastasis have a larger stage number and a worse prognosis.
The main stages are:- Stage 0 is a pre-cancerous or marker condition, either ductal carcinoma in situ (DCIS) or lobular carcinoma in situ (LCIS).
- Stages 1–3 are defined as 'early' cancer with a good prognosis.
- Stage 4 is defined as 'advanced' and/or 'metastatic' cancer with a poor prognosis.
- Histopathology. Breast cancer is usually classified primarily by its histological appearance. Most breast cancers are derived from the epithelium lining the ducts or lobules, and these cancers are classified as ductal or lobular carcinoma. Carcinoma in situ is growth of low grade cancerous or precancerous cells in particular tissue compartment such as the mammary duct without invasion of the surrounding tissue. In contrast, invasive carcinoma does not confine itself to the initial tissue compartment and invades the surrounding tissue.[8]
- Grade (Bloom-Richardson grade). When cells become differentiated, they take different shapes and forms to function as part of an organ. Cancerous cells lose that differentiation. In cancer grading, tumor cells are generally classified as well differentiated (low grade), moderately differentiated (intermediate grade), and poorly differentiated (high grade). Poorly differentiated cancers have a worse prognosis.
- Receptor status. Cells have receptors on their surface and in their cytoplasm and nucleus. Chemical messengers such as hormones bind to these receptors, and this causes changes in the cell. Breast cancer cells may or may not have three important receptors: estrogen receptor (ER), progesterone receptor (PR), and HER2/neu.
ER+ cancer cells depend on estrogen for their growth, so they can be treated with drugs to block estrogen effects (e.g. tamoxifen), and generally have a better prognosis.
HER2+ breast cancer had a worse prognosis,[9] but HER2+ cancer cells respond to drugs such as the monoclonal antibody, trastuzumab, (in combination with conventional chemotherapy) and this has improved the prognosis significantly.[10] Cells with none of these receptors are called basal-like or triple negative. - DNA assays of various types including DNA microarrays have compared normal cells to breast cancer cells. The specific changes in a particular breast cancer can be used to classify the cancer in several ways, and may assist in choosing the most effective treatment for that DNA type.
Signs and symptoms

The first noticeable symptom of breast cancer is typically a lump that feels different from the rest of the breast tissue. More than 80% of breast cancer cases are discovered when the woman feels a lump.[11] The earliest breast cancers are detected by a mammogram.[12] Lumps found in lymph nodes located in the armpits[11] can also indicate breast cancer.
Indications of breast cancer other than a lump may include changes in breast size or shape, skin dimpling, nipple inversion, or spontaneous single-nipple discharge. Pain ("mastodynia") is an unreliable tool in determining the presence or absence of breast cancer, but may be indicative of other breast health issues.[11][12][13]
Inflammatory breast cancer is a special type of breast cancer which can pose a substantial diagnostic challenge. Symptoms may resemble a breast inflammation and may include pain, swelling, nipple inversion, warmth and redness throughout the breast, as well as an orange-peel texture to the skin referred to as peau d'orange.[11]
Another reported symptom complex of breast cancer is Paget's disease of the breast. This syndrome presents as eczematoid skin changes such as redness and mild flaking of the nipple skin. As Paget's advances, symptoms may include tingling, itching, increased sensitivity, burning, and pain. There may also be discharge from the nipple. Approximately half of women diagnosed with Paget's also have a lump in the breast.[14]
In rare cases, what initially appears as a fibroadenoma (hard movable lump) could in fact be a phyllodes tumor. Phyllodes tumors are formed within the stroma (connective tissue) of the breast and contain glandular as well as stromal tissue. Phyllodes tumors are not staged in the usual sense; they are classified on the basis of their appearance under the microscope as benign, borderline, or malignant.[15]
Occasionally, breast cancer presents as metastatic disease, that is, cancer that has spread beyond the original organ. Metastatic breast cancer will cause symptoms that depend on the location of metastasis. Common sites of metastasis include bone, liver, lung and brain.[16] Unexplained weight loss can occasionally herald an occult breast cancer, as can symptoms of fevers or chills. Bone or joint pains can sometimes be manifestations of metastatic breast cancer, as can jaundice or neurological symptoms. These symptoms are "non-specific", meaning they can also be manifestations of many other illnesses.[17]
Most symptoms of breast disorder do not turn out to represent underlying breast cancer. Benign breast diseases such as mastitis and fibroadenoma of the breast are more common causes of breast disorder symptoms. The appearance of a new symptom should be taken seriously by both patients and their doctors, because of the possibility of an underlying breast cancer at almost any age.[18]
Risk factors
The primary risk factors for breast cancer are sex,[19] age,[20] lack of childbearing or breastfeeding,[21] higher hormone levels,[22][23] race, economic status and dietary iodine deficiency.[24][25][26]
Most cases of breast cancer cannot be prevented through any action on the part of the affected person. The World Cancer Research Fund estimated that 38% of breast cancer cases in the US are preventable through reducing alcohol intake, increasing physical activity levels and maintaining a healthy weight.[27] It also estimated that 42% of breast cancer cases in the UK could be prevented in this way, as well as 28% in Brazil and 20% in China.
Smoking tobacco also increases the risk of breast cancer with the greater the amount smoking and the earlier in life smoking begins the higher the risk.[28]
In a study of attributable risk and epidemiological factors published in 1995, later age at first birth and not having children accounted for 29.5% of U.S. breast cancer cases, family history of breast cancer accounted for 9.1% and factors correlated with higher income contributed 18.9% of cases.[29] Attempts to explain the increased incidence (but lower mortality) correlated with higher income include epidemiologic observations such as lower birth rates correlated with higher income and better education, possible overdiagnosis and overtreatment because of better access to breast cancer screening, and the postulation of as yet unexplained lifestyle and dietary factors correlated with higher income. One such factor may be past hormone replacement therapy, which was typically more widespread in higher income groups.
Genetic factors usually increase the risk slightly or moderately; the exception is women and men who are carriers of BRCA mutations. These people have a very high lifetime risk for breast and ovarian cancer, depending on the portion of the proteins where the mutation occurs. Instead of a 12 percent lifetime risk of breast cancer, women with one of these genes have a risk of approximately 60 percent.[30]
In more recent years, research has indicated the impact of diet and other behaviors on breast cancer. These additional risk factors include a high-fat diet,[31] alcohol intake,[32] obesity,[33] and environmental factors such as tobacco use, radiation,[34] endocrine disruptors and shiftwork.[35] Although the radiation from mammography is a low dose, the cumulative effect can cause cancer.[36] [37]
In addition to the risk factors specified above, demographic and medical risk factors include:
- Personal history of breast cancer: A woman who had breast cancer in one breast has an increased risk of getting a second breast cancer.
- Family history: A woman's risk of breast cancer is higher if her mother, sister, or daughter had breast cancer, the risk becomes significant if at least two close relatives had breast or ovarian cancer. The risk is higher if her family member got breast cancer before age 40. An Australian study found that having other relatives with breast cancer (in either her mother's or father's family) may also increase a woman's risk of breast cancer and other forms of cancer, including brain and lung cancers.[38]
- Certain breast changes: Atypical hyperplasia and lobular carcinoma in situ found in benign breast conditions such as fibrocystic breast changes are correlated with an increased breast cancer risk.
Those with a normal body mass index at age 20 who gained weight as they aged had nearly double the risk of developing breast cancer after menopause in comparison to women who maintained their weight. The average 60-year-old woman's risk of developing breast cancer by age 65 is about 2 percent; her lifetime risk is 13 percent.[39]
A 2011 study done at the University of Rochester Medical Center found that low vitamin D levels among women with breast cancer correlate with more aggressive tumors and poorer prognosis. The study associated sub-optimal vitamin D levels with poor scores on every major biological marker that helps physicians predict a patient’s breast cancer outcome. The lead researcher stated, “Based on these results, doctors should strongly consider monitoring vitamin D levels among breast cancer patients and correcting them as needed.”[40]
Prevention
Masturbation can help decrease risk for Breast cancer. Exercise may decrease breast cancer risk.[41] Also avoiding alcohol and obesity. Prophylactic bilateral mastectomy may be considered in patients with BRCA1 and BRCA2 mutations.[42][43] A 2007 report concluded that women can somewhat reduce their risk by maintaining a healthy weight, drinking less alcohol, being physically active and breastfeeding their children.[44]
Pathophysiology
Breast cancer, like other cancers, occurs because of an interaction between the environment and a defective gene. Normal cells divide as many times as needed and stop. They attach to other cells and stay in place in tissues. Cells become cancerous when mutations destroy their ability to stop dividing, to attach to other cells and to stay where they belong. When cells divide, their DNA is normally copied with many mistakes. Error-correcting proteins fix those mistakes. The mutations known to cause cancer, such as p53, BRCA1 and BRCA2, occur in the error-correcting mechanisms. These mutations are either inherited or acquired after birth. Presumably, they allow the other mutations, which allow uncontrolled division, lack of attachment, and metastasis to distant organs.[34][45] Normal cells will commit cell suicide (apoptosis) when they are no longer needed. Until then, they are protected from cell suicide by several protein clusters and pathways. One of the protective pathways is the PI3K/AKT pathway; another is the RAS/MEK/ERK pathway. Sometimes the genes along these protective pathways are mutated in a way that turns them permanently "on", rendering the cell incapable of committing suicide when it is no longer needed. This is one of the steps that causes cancer in combination with other mutations. Normally, the PTEN protein turns off the PI3K/AKT pathway when the cell is ready for cell suicide. In some breast cancers, the gene for the PTEN protein is mutated, so the PI3K/AKT pathway is stuck in the "on" position, and the cancer cell does not commit suicide.[46]
Mutations that can lead to breast cancer have been experimentally linked to estrogen exposure.[47]
Failure of immune surveillance, the removal of malignant cells throughout one's life by the immune system.[48]
Abnormal growth factor signaling in the interaction between stromal cells and epithelial cells can facilitate malignant cell growth.[49][50]
In the United States, 10 to 20 percent of patients with breast cancer and patients with ovarian cancer have a first- or second-degree relative with one of these diseases. Mutations in either of two major susceptibility genes, breast cancer susceptibility gene 1 (BRCA1) and breast cancer susceptibility gene 2 (BRCA2), confer a lifetime risk of breast cancer of between 60 and 85 percent and a lifetime risk of ovarian cancer of between 15 and 40 percent. However, mutations in these genes account for only 2 to 3 percent of all breast cancers.[51]
Diagnosis
While screening techniques (which are further discussed below) are useful in determining the possibility of cancer, a further testing is necessary to confirm whether a lump detected on screening is cancer, as opposed to a benign alternative such as a simple cyst.
Very often the results of noninvasive examination, mammography and additional tests that are performed in special circumstances such as ultrasound or MR imaging are sufficient to warrant excisional biopsy as the definitive diagnostic and curative method.
Both mammography and clinical breast exam, also used for screening, can indicate an approximate likelihood that a lump is cancer, and may also detect some other lesions.[52] When the tests are inconclusive Fine Needle Aspiration and Cytology (FNAC) may be used. FNAC may be done in a GP's office using local anaesthetic if required, involves attempting to extract a small portion of fluid from the lump. Clear fluid makes the lump highly unlikely to be cancerous, but bloody fluid may be sent off for inspection under a microscope for cancerous cells. Together, these three tools can be used to diagnose breast cancer with a good degree of accuracy.
Other options for biopsy include core biopsy, where a section of the breast lump is removed, and an excisional biopsy, where the entire lump is removed.
In addition vacuum-assisted breast biopsy (VAB) may help diagnose breast cancer among patients with a mammographically detected breast in women.[53]
-

-
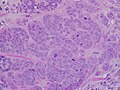 High grade invasive ductal carcinoma, with minimal tubule formation, marked pleomorphism, and prominent mitoses, 40x field.
High grade invasive ductal carcinoma, with minimal tubule formation, marked pleomorphism, and prominent mitoses, 40x field. -
 Micrograph showing a lymph node invaded by ductal breast carcinoma and with extranodal extension of tumour.
Micrograph showing a lymph node invaded by ductal breast carcinoma and with extranodal extension of tumour. -
 Neuropilin-2 expression in normal breast and breast carcinoma tissue.
Neuropilin-2 expression in normal breast and breast carcinoma tissue. -
 Lymph nodes which drain the breast
Lymph nodes which drain the breast -
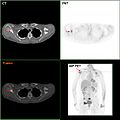 F-18 FDG PET/CT: Metastasis of a mamma carcinoma in the right scapula
F-18 FDG PET/CT: Metastasis of a mamma carcinoma in the right scapula



_expression_in_normal_breast_and_breast_carcinoma_tissue.jpg)


Screening
Breast cancer screening refers to testing otherwise-healthy women for breast cancer in an attempt to achieve an earlier diagnosis. The assumption is that early detection will improve outcomes. A number of screening test have been employed including: clinical and self breast exams, mammography, genetic screening, ultrasound, and magnetic resonance imaging.
A clinical or self breast exam involves feeling the breast for lumps or other abnormalities. Research evidence does not support the effectiveness of either type of breast exam, because by the time a lump is large enough to be found it is likely to have been growing for several years and will soon be large enough to be found without an exam.[54] Mammographic screening for breast cancer uses x-rays to examine the breast for any uncharacteristic masses or lumps. The Cochrane collaboration in 2009 concluded that mammograms reduce mortality from breast cancer by 15 percent but also result in unnecessary surgery and anxiety, resulting in their view that it is not clear whether mammography screening does more good or harm.[55] Many national organizations recommend regular mammography, nevertheless. For the average woman, the U.S. Preventive Services Task Force recommends mammography every two years in women between the ages of 50 and 74.[56] The Task Force points out that in addition to unnecessary surgery and anxiety, the risks of more frequent mammograms include a small but significant increase in breast cancer induced by radiation.[57]
In women at high risk, such as those with a strong family history of cancer, mammography screening is recommended at an earlier age and additional testing may include genetic screening that tests for the BRCA genes and / or magnetic resonance imaging. Molecular breast imaging is currently under study and may also be an alternative.[58]
Treatment
Breast cancer is usually treated with surgery and then possibly with chemotherapy or radiation, or both. Hormone positive cancers are treated with long term hormone blocking therapy. Treatments are given with increasing aggressiveness according to the prognosis and risk of recurrence.
- Stage 1 cancers (and DCIS) have an excellent prognosis and are generally treated with lumpectomy and sometimes radiation.[59] HER2+ cancers should be treated with the trastuzumab (Herceptin) regime.[60] Chemotherapy is uncommon for other types of stage 1 cancers.
- Stage 2 and 3 cancers with a progressively poorer prognosis and greater risk of recurrence are generally treated with surgery (lumpectomy or mastectomy with or without lymph node removal), chemotherapy (plus trastuzumab for HER2+ cancers) and sometimes radiation (particularly following large cancers, multiple positive nodes or lumpectomy).
- Stage 4, metastatic cancer, (i.e. spread to distant sites) has poor prognosis and is managed by various combination of all treatments from surgery, radiation, chemotherapy and targeted therapies. 10 year survival rate is 5% without treatment and 10% with optimal treatment.[61]
Medications


Drugs used after and in addition to surgery are called adjuvant therapy. Chemotherapy prior to surgery is called neo-adjuvant therapy. There are currently 3 main groups of medications used for adjuvant breast cancer treatment:
- Hormone blocking therapy
- Chemotherapy
- Monoclonal antibodies
One or all of these groups can be used.
Hormone Blocking Therapy: Some breast cancers require estrogen to continue growing. They can be identified by the presence of estrogen receptors (ER+) and progesterone receptors (PR+) on their surface (sometimes referred to together as hormone receptors). These ER+ cancers can be treated with drugs that either block the receptors, e.g. tamoxifen, or alternatively block the production of estrogen with an aromatase inhibitor, e.g. anastrozole (Arimidex) or letrozole (Femara). Aromatase inhibitors, however, are only suitable for post-menopausal patients.
Chemotherapy: Predominately used for stage 2-4 disease, being particularly beneficial in estrogen receptor-negative (ER-) disease. They are given in combinations, usually for 3–6 months. One of the most common treatments is cyclophosphamide plus doxorubicin (Adriamycin), known as AC. The mechanism of action of chemotherapy is to destroy fast growing an or fast replicating cancer cells either by causing DNA damage upon replication or other mechanisms; these drugs also damage fast-growing normal cells where they cause serious side effects. Damage to the heart muscle is the most dangerous complication of doxorubicin. Sometimes a taxane drug, such as docetaxel, is added, and the regime is then known as CAT; taxane attacks the microtubules in cancer cells. Another common treatment, which produces equivalent results, is cyclophosphamide, methotrexate, and fluorouracil (CMF). (Chemotherapy can literally refer to any drug, but it is usually used to refer to traditional non-hormone treatments for cancer.)
Monoclonal antibodies: A relatively recent development in HER2+ breast cancer treatment. Approximately 15-20 percent of breast cancers have an amplification of the HER2/neu gene or overexpression of its protein product.[62] This receptor is normally stimulated by a growth factor which causes the cell to divide; in the absence of the growth factor, the cell will normally stop growing. Overexpression of this receptor in breast cancer is associated with increased disease recurrence and worse prognosis. Trastuzumab (Herceptin), a monoclonal antibody to HER2, has improved the 5 year disease free survival of stage 1–3 HER2+ breast cancers to about 87% (overall survival 95%).[63] Trastuzumab, however, is expensive, and approx 2% of patients suffer significant heart damage; it is otherwise well tolerated, with far milder side effects than conventional chemotherapy.[64] Other monoclonal antibodies are also undergoing clinical trials.
A recent analysis of a subset of the Nurses' Health Study data indicated that Aspirin may reduce mortality from breast cancer.[65]
Radiation
Radiotherapy is given after surgery to the region of the tumor bed and regional lymph nodes, to destroy microscopic tumor cells that may have escaped surgery. It may also have a beneficial effect on tumor microenvironment.[66][67] Radiation therapy can be delivered as external beam radiotherapy or as brachytherapy (internal radiotherapy). Conventionally radiotherapy is given after the operation for breast cancer. Radiation can also be given at the time of operation on the breast cancer- intraoperatively. The largest randomised trial to test this approach was the TAR-GIT-A Trial[68] which found that targeted intraoperative radiotherapy was equally effective at 4-years as the usual several weeks' of whole breast external beam radiotherapy.[69] Radiation can reduce the risk of recurrence by 50-66% (1/2 - 2/3 reduction of risk) when delivered in the correct dose[70] and is considered essential when breast cancer is treated by removing only the lump (Lumpectomy or Wide local excision)
Prognosis
A prognosis is a prediction of outcome and the probability of progression-free survival (PFS) or disease-free survival (DFS). These predictions are based on experience with breast cancer patients with similar classification. A prognosis is an estimate, as patients with the same classification will survive a different amount of time, and classifications are not always precise. Survival is usually calculated as an average number of months (or years) that 50% of patients survive, or the percentage of patients that are alive after 1, 5, 15, and 20 years. Prognosis is important for treatment decisions because patients with a good prognosis are usually offered less invasive treatments, such as lumpectomy and radiation or hormone therapy, while patients with poor prognosis are usually offered more aggressive treatment, such as more extensive mastectomy and one or more chemotherapy drugs.
Prognostic factors include staging, (i.e., tumor size, location, grade, whether disease has spread to other parts of the body), recurrence of the disease, and age of patient.
Stage is the most important, as it takes into consideration size, local involvement, lymph node status and whether metastatic disease is present. The higher the stage at diagnosis, the poorer the prognosis. The stage is raised by the invasiveness of disease to lymph nodes, chest wall, skin or beyond, and the aggressiveness of the cancer cells. The stage is lowered by the presence of cancer-free zones and close-to-normal cell behaviour (grading). Size is not a factor in staging unless the cancer is invasive. For example, Ductal Carcinoma In Situ (DCIS) involving the entire breast will still be stage zero and consequently an excellent prognosis with a 10yr disease free survival of about 98%.[71]
Grading is based on how biopsied, cultured cells behave. The closer to normal cancer cells are, the slower their growth and the better the prognosis. If cells are not well differentiated, they will appear immature, will divide more rapidly, and will tend to spread. Well differentiated is given a grade of 1, moderate is grade 2, while poor or undifferentiated is given a higher grade of 3 or 4 (depending upon the scale used). The most widely used grading system is the Nottingham Modification of the Bloom-Richardson system,[72] which grades breast carcinomas by adding up scores for tubule formation, nuclear pleomorphism, and mitotic count, each of which is given 1 to 3 points, which add to a final score as follows: 3-5 points = Grade I; 6-7 points = Grade II; and 8-9 points = Grade III. The grading criteria is as follows:
Tubule formation
- 1 point: tubular formation in >75% of the tumor
- 2 points: tubular formation in 10 to 75% of the tumor
- 3 points: tubular formation in <10% of the tumor
Note: The overall appearance of the tumor has to be considered.
Nuclear pleomorphism
- 1 point: nuclei with mimimal variation in size and shape
- 2 points: nuclei with moderate variation in size and shape
- 3 points: nuclei with marked variation in size and shape
Note: The tumor areas having cells with the greatest atypia should be evaluated.
Mitotic count
- 1 point: 0-9 mitotic counts per field under X25 objective using the Leitz Ortholux microscope, 0-5 mitotic counts per field under X40 objective using the Nikon Labophot microscope, or 0-11 mitotic counts per field under X40 objective using the Leitz Daiplan microscope
- 2 points: 10-19 mitotic counts per field under X25 objective using the Leitz Ortholux microscope, 6-10 mitotic counts per field under X40 objective using the Nikon Labophot microscope, or 12-22 mitotic counts per field under X40 objective using the Leitz Daiplan microscope
- 3 points: >19 mitotic counts per field under X25 objective using the Leitz Ortholux microscope, >10 mitotic counts per field under X40 objective using the Nikon Labophot microscope, or >22 mitotic counts per field under X40 objective using the Leitz Daiplan microscope
Note: Mitotic figures are counted only at the periphery of the tumor, and counting should begin in the most mitotically active areas.
Younger women tend to have a poorer prognosis than post-menopausal women due to several factors. Their breasts are active with their cycles, they may be nursing infants, and may be unaware of changes in their breasts. Therefore, younger women are usually at a more advanced stage when diagnosed. There may also be biologic factors contributing to a higher risk of disease recurrence for younger women with breast cancer.[73]
The presence of estrogen and progesterone receptors in the cancer cell is important in guiding treatment. Those who do not test positive for these specific receptors will not be able to respond to hormone therapy, and this can affect their chance of survival depending upon what treatment options remain, the exact type of the cancer, and how advanced the disease is.
In addition to hormone receptors, there are other cell surface proteins that may affect prognosis and treatment. HER2 status directs the course of treatment. Patients whose cancer cells are positive for HER2 have more aggressive disease and may be treated with the 'targeted therapy', trastuzumab (Herceptin), a monoclonal antibody that targets this protein and improves the prognosis significantly. Tumors overexpressing the Wnt signaling pathway co-receptor low-density lipoprotein receptor-related protein 6 (LRP6) may represent a distinct subtype of breast cancer and a potential treatment target.[74]
Psychological aspects
The emotional impact of cancer diagnosis, symptoms, treatment, and related issues can be severe. Most larger hospitals are associated with cancer support groups which provide a supportive environment to help patients cope and gain perspective from cancer survivors. Online cancer support groups are also very beneficial to cancer patients, especially in dealing with uncertainty and body-image problems inherent in cancer treatment.
Not all breast cancer patients experience their illness in the same manner. Factors such as age can have a significant impact on the way a patient copes with a breast cancer diagnosis. Premenopausal women with estrogen-receptor positive breast cancer must confront the issues of early menopause induced by many of the chemotherapy regimens used to treat their breast cancer, especially those that use hormones to counteract ovarian function.[75]
On the other hand, a recent study conducted by researchers at the College of Public Health of the University of Georgia showed that older women may face a more difficult recovery from breast cancer than their younger counterparts.[76] As the incidence of breast cancer in women over 50 rises and survival rates increase, breast cancer is increasingly becoming a geriatric issue that warrants both further research and the expansion of specialized cancer support services tailored for specific age groups.[76]
Epidemiology

Worldwide, breast cancer is the most common invasive cancer in women. (The most common form of cancer is non-invasive non-melanoma skin cancer; non-invasive cancers are generally easily cured, cause very few deaths, and are routinely excluded from cancer statistics.) Breast cancer comprises 22.9% of invasive cancers in women[6] and 16% of all female cancers.[78]
In 2008, breast cancer caused 458,503 deaths worldwide (13.7% of cancer deaths in women and 6.0% of all cancer deaths for men and women together).[6] Lung cancer, the second most common cause of cancer-related death in women, caused 12.8% of cancer deaths in women (18.2% of all cancer deaths for men and women together).[6]
The incidence of breast cancer varies greatly around the world: it is lowest in less-developed countries and greatest in the more-developed countries. In the twelve world regions, the annual age-standardized incidence rates per 100,000 women are as follows: in Eastern Asia, 18; South Central Asia, 22; sub-Saharan Africa, 22; South-Eastern Asia, 26; North Africa and Western Asia, 28; South and Central America, 42; Eastern Europe, 49; Southern Europe, 56; Northern Europe, 73; Oceania, 74; Western Europe, 78; and in North America, 90.[79]
The number of cases worldwide has significantly increased since the 1970s, a phenomenon partly attributed to the modern lifestyles.[80][81]
Breast cancer is strongly related to age with only 5% of all breast cancers occurring in women under 40 years old.[82]
United States


The lifetime risk for breast cancer in the United States is usually given as about 1 in 8 (12%) of women by age 95, with a 1 in 35 (3%) chance of dying from breast cancer.[84] This calculation assumes that all women live to at least age 95, except for those who die from breast cancer before age 95.[85] Recent work, using real-world numbers, indicate that the actual risk is probably less than half the theoretical risk.[86]
The United States has the highest annual incidence rates of breast cancer in the world; 128.6 per 100,000 in whites and 112.6 per 100,000 among African Americans.[84][87] It is the second-most common cancer (after skin cancer) and the second-most common cause of cancer death (after lung cancer).[84] In 2007, breast cancer was expected to cause 40,910 deaths in the US (7% of cancer deaths; almost 2% of all deaths).[12] This figure includes 450-500 annual deaths among men out of 2000 cancer cases.[88]
In the US, both incidence and death rates for breast cancer have been declining in the last few years in Native Americans and Alaskan Natives.[12][89] Nevertheless, a US study conducted in 2005 indicated that breast cancer remains the most feared disease,[90] even though heart disease is a much more common cause of death among women.[91] Many doctors say that women exaggerate their risk of breast cancer.[92]
UK
45,000 cases diagnosed and 12,500 deaths per annum.[93]
Developing countries
As developing countries grow and adopt Western culture they also accumulate more disease that has arisen from Western culture and its habits (fat/alcohol intake, smoking, exposure to oral contraceptives, the changing patterns of childbearing and breastfeeding, low parity). For instance, as South America has developed so has the amount of breast cancer. "Breast cancer in less developed countries, such as those in South America, is a major public health issue. It is a leading cause of cancer-related deaths in women in countries such as Argentina, Uruguay, and Brazil. The expected numbers of new cases and deaths due to breast cancer in South America for the year 2001 are approximately 70,000 and 30,000, respectively." [94] However, because of a lack of funding and resources, treatment is not always available to those suffering with breast cancer.
History

Because of its visibility, breast cancer was the form of cancer most often described in ancient documents.[95] Because autopsies were rare, cancers of the internal organs were essentially invisible to ancient medicine. Breast cancer, however, could be felt through the skin, and in its advanced state often developed into fungating lesions: the tumor would become necrotic (die from the inside, causing the tumor to appear to break up) and ulcerate through the skin, weeping fetid, dark fluid.[95]
The oldest description of cancer was discovered in Egypt and dates back to approximately 1600 BC. The Edwin Smith Papyrus describes 8 cases of tumors or ulcers of the breast that were treated by cauterization. The writing says about the disease, "There is no treatment."[96] For centuries, physicians described similar cases in their practises, with the same conclusion. Ancient medicine, from the time of the Greeks through the 17th century, was based on humoralism, and thus believed that breast cancer was generally caused by imbalances in the fundamental fluids that controlled the body, especially an excess of black bile.[97] Alternatively, patients often saw it as divine punishment.[98] In the 18th century, a wide variety of medical explanations were proposed, including a lack of sexual activity, too much sexual activity, physical injuries to the breast, curdled breast milk, and various forms of lymphatic blockages, either internal or due to restrictive clothing.[97][99] In the 19th century, the Scottish surgeon John Rodman said that fear of cancer caused cancer, and that this anxiety, learned by example from the mother, accounted for breast cancer's tendency to run in families.[99]
Although breast cancer was known in ancient times, it was uncommon until the 19th century, when improvements in sanitation and control of deadly infectious diseases resulted in dramatic increases in lifespan. Previously, most women had died too young to have developed breast cancer.[99] Additionally, early and frequent childbearing and breastfeeding probably reduced the rate of breast cancer development in those women who did survive to middle age.[99]
Because ancient medicine believed that the cause was systemic, rather than local, and because surgery carried a high mortality rate, the preferred treatments tended to be pharmacological rather than surgical. Herbal and mineral preparations, especially involving the poisons hemlock or arsenic, were relatively common.
Mastectomy for breast cancer was performed at least as early as 548 CE, when it was proposed by the court physician Aetios of Amida to Theodora.[95] It was not until doctors achieved greater understanding of the circulatory system in the 17th century that they could link breast cancer's spread to the lymph nodes in the armpit. The French surgeon Jean Louis Petit (1674–1750) and later the Scottish surgeon Benjamin Bell (1749–1806) were the first to remove the lymph nodes, breast tissue, and underlying chest muscle.[100]
Their successful work was carried on by William Stewart Halsted who started performing radical mastectomies in 1882, helped greatly by advances in general surgical technology, such as aseptic technique and anesthesia. The Halsted radical mastectomy often involved removing both breasts, associated lymph nodes, and the underlying chest muscles. This often led to long-term pain and disability, but was seen as necessary in order to prevent the cancer from recurring.[101] Before the advent of the Halsted radical mastectomy, 20-year survival rates were only 10%; Halsted's surgery raised that rate to 50%.[102] Extending Halsted's work, Jerome Urban promoted superradical mastectomies, taking even more tissue, until 1963, when the ten-year survival rates proved equal to the less-damaging radical mastectomy.[101]
Radical mastectomies remained the standard of care in America until the 1970s, but in Europe, breast-sparing procedures, often followed radiation therapy, were generally adopted in the 1950s.[101] One reason for this striking difference in approach may be the structure of the medical professions: European surgeons, descended from the barber surgeon, were held in less esteem than physicians; in America, the surgeon was the king of the medical profession.[101] Additionally, there were far more European women surgeons: Less than one percent of American surgical oncologists were female, but some European breast cancer wards boasted a medical staff that was half female.[101] American health insurance companies also paid surgeons more to perform radical mastectomies than they did to perform more intricate breast-sparing surgeries.[101]
Breast cancer staging systems were developed in the 1920s and 1930s.[101]
During the 1970s, a new understanding of metastasis led to perceiving cancer as a systemic illness as well as a localized one, and more sparing procedures were developed that proved equally effective. Modern chemotherapy developed after World War II.[103]
The French surgeon Bernard Peyrilhe (1737–1804) realized the first experimental transmission of cancer by injecting extracts of breast cancer into an animal.
Prominent women who died of breast cancer include Anne of Austria, the mother of Louis XIV of France; Mary Washington, mother of George, and Rachel Carson, the environmentalist.[104]
The first case-controlled study on breast cancer epidemiology was done by Janet Lane-Claypon, who published a comparative study in 1926 of 500 breast cancer cases and 500 control patients of the same background and lifestyle for the British Ministry of Health.[105][verification needed][106]
In the 1980s and 1990s, thousands of women who had successfully completed standard treatment then demanded and received high-dose bone marrow transplants, thinking this would lead to better long-term survival. However, it proved completely ineffective, and 15–20% of women died because of the brutal treatment.[107]
The 1995 reports from the Nurses' Health Study and the 2002 conclusions of the Women's Health Initiative trial conclusively proved that hormone replacement therapy significantly increased the incidence of breast cancer.[107]
Society and culture
Before the 20th century, breast cancer was feared and discussed in hushed tones, as if it were shameful. As little could be safely done with primitive surgical techniques, women tended to suffer silently rather than seeking care. When surgery advanced, and long-term survival rates improved, women began raising awareness of the disease and the possibility of successful treatment. The "Women's Field Army", run by the American Society for the Control of Cancer (the forerunner of the American Cancer Society) during the 1930s and 1940s was one of the first organized campaigns. In 1952, the first peer-to-peer support group, called "Reach to Recovery", began providing post-mastectomy, in-hospital visits from women who had survived breast cancer.[108]
The breast cancer movement of the 1980s and 1990s developed out of the larger feminist movements and women's health movement of the 20th century.[109] This series of political and educational campaigns, partly inspired by the politically and socially effective AIDS awareness campaigns, resulted in the widespread acceptance of second opinions before surgery, less invasive surgical procedures, support groups, and other advances in patient care.[110]
Awareness Month
In most countries, October is recognized as National Breast Cancer Awareness Month (NBCAM). The primary purpose is to promote screening mammography as the most effective way to save lives by detecting breast cancer at early stages.[111]
The month features many events, especially fundraisers. Cosmetics company Estée Lauder has sponsored the illumination of landmarks with pink lights. Lee National Denim Day encourages employers to offer a relaxed dress code in return for a small donation to a breast cancer charity. Susan G. Komen for the Cure and other breast cancer organizations hold walkathons and other sponsored athletic events. The ubiquitous presence of pink ribbons and other pink objects has prompted the title "Pinktober". Typically, relatively little money from pink ribbons and tie-in merchandise is donated to the cause.[112]
Some critics call NBCAM the "National Breast Cancer Industry Month" to highlight the conflict of interest between corporations promoting breast cancer awareness while profiting from the resulting increased diagnoses and treatments. Breast Cancer Action says that October is a slick public relations campaign that distracts people from discovering the causes and means of preventing breast cancer and instead focuses on raising awareness as a way to sell mammography equipment and chemotherapy drugs. The term pinkwashing describes the actions of companies that manufacture and use chemicals which may cause breast cancer while simultaneously and hypocritically giving money to breast cancer organizations.[113]
Pink ribbon

A pink ribbon is the most prominent symbol of breast cancer awareness. Pink ribbons, which can be made inexpensively, are sometimes sold as fundraisers, much like poppies on Remembrance Day. They may be worn to honor those who have been diagnosed with breast cancer, or to identify products that the manufacturer would like to sell to consumers that are interested in breast cancer—usually white, middle-aged, middle-class, educated women.
The pink ribbon is associated with individual generosity, faith in scientific progress, and a "can-do" attitude. It encourages consumers to focus on the emotionally appealing ultimate vision of a cure for breast cancer, rather than on the fraught path between current knowledge and any future cures.[114]
Promotion of the pink ribbon as a symbol for breast cancer has not been credited with saving any lives. Wearing or displaying a pink ribbon has been denounced as a kind of slacktivism, because it has no practical positive effect and as hypocrisy among those who wear the pink ribbon to show good will towards women with breast cancer, but then oppose these women's practical goals, like patient rights and anti-pollution legislation.[115][116] Critics say that the feel-good nature of pink ribbons and pink consumption distracts society from the lack of progress on preventing and curing breast cancer.[117] It is also criticized for reinforcing gender stereotypes and objectifying women and their breasts.[118] Breast Cancer Action launched the "Think Before You Pink" campaign, and charged that companies have co-opted the pink campaign to promote products that encourage breast cancer, such as high-fat Kentucky Fried Chicken and alcohol.[119]
Breast cancer culture
Breast cancer culture, or pink ribbon culture, is the set of activities, attitudes, and values that surround and shape breast cancer in public. The dominant values are selflessness, cheerfulness, unity, and optimism. Appearing to have suffered bravely is the passport into the culture.
The woman with breast cancer is given a cultural template that constrains her emotional and social responses into a socially acceptable discourse: She is to use the emotional trauma of being diagnosed with breast cancer and the suffering of extended treatment to transform herself into a stronger, happier and more sensitive person who is grateful for the opportunity to become a better person. Breast cancer thereby becomes a rite of passage rather than a disease.[120] To fit into this mold, the woman with breast cancer needs to normalize and feminize her appearance, and minimize the disruption that her health issues cause anyone else. Anger, sadness and negativity must be silenced.[120]
As with most cultural models, people who conform to the model are given social status, in this case as cancer survivors. Women who reject the model are shunned, punished and shamed.[120]
The culture is criticized for treating adult women like little girls, as evidenced by "baby" toys such as pink teddy bears given to adult women.[120]
The primary purposes or goals of breast cancer culture are to maintain breast cancer's dominance as the preëminent women's health issue, to promote the appearance that society is "doing something" effective about breast cancer, and to sustain and expand the social, political, and financial power of breast cancer activists.[121]
Overemphasis?
Compared to other diseases or other cancers, breast cancer receives a disproportionate share of resources and attention. In 2001 MP Ian Gibson, chairman of the UK House of Commons all party group on cancer stated "The treatment has been skewed by the lobbying, there is no doubt about that. Breast cancer sufferers get better treatment in terms of bed spaces, facilities and doctors and nurses."[122] Breast cancer also receives significantly more media coverage than other, equally prevalent cancers, with a study by Prostate Coalition showing 2.6 breast cancer stories for each one covering cancer of the prostate.[123] Ultimately there is a concern that favoring sufferers of breast cancer with disproporionate research on their behalf may well be costing lives elsewhere.[122] Partly because of its relatively high prevalence and long-term survival rates, research is biased towards breast cancer. Some subjects, such as cancer-related fatigue, have been studied in little except women with breast cancer.
One result of breast cancer's high visibility is that most women significantly overestimate their personal risk of dying from it. Misleading statistics, such as the claim that one in eight women will be diagnosed with breast cancer during their lives—a claim that depends on the patently unrealistic assumption that no woman will die of any other disease before the age of 95[85]—obscure the reality, which is that about ten times as many women will die from heart disease or stroke than from breast cancer.[124]
The emphasis on breast cancer screening may be harming women by subjecting them to unnecessary radiation, biopsies, and surgery. One-third of diagnosed breast cancers might recede on their own.[125] Screening mammography efficiently finds non-life-threatening, asymptomatic breast cancers and pre-cancers, even while overlooking serious cancers. According to H. Gilbert Welch of the Dartmouth Institute for Health Policy and Clinical Practice, research on screening mammography has taken the "brain-dead approach that says the best test is the one that finds the most cancers" rather than the one that finds dangerous cancers.[125]
Art
Several historical paintings show anomalies that have been interpreted as visible evidence of breast cancer; retrospective diagnoses are discussed in the medical literature. Possible signs of breast cancer such as a typical lump, differences in breast size or shape and the peau d'orange skin texture can be found for example in works by Raphael, Rembrandt and Rubens.[95][126][127][128]
The paintings and the historical context do not give enough information to conclude whether or not the visible changes are really signs of breast cancer[129] and alternative explanations such as tuberculous mastitis or a chronic lactational breast abscess need to be considered.[130]
- Examples of breast cancer signs in art
-
 Raffaelo Sanzio (1483–1520): Portrait of a young woman (La Fornarina)
Raffaelo Sanzio (1483–1520): Portrait of a young woman (La Fornarina) -
 Peter Paul Rubens (1577–1640): The Three Graces
Peter Paul Rubens (1577–1640): The Three Graces -
 Rembrandt van Rijn (1606–1669): Bathsheba with King David's Letter
Rembrandt van Rijn (1606–1669): Bathsheba with King David's Letter -
 details
details -

-







Research
A considerable part of the current knowledge on breast carcinomas is based on in vivo and in vitro studies performed with breast cancer cell (BCC) lines. These provide an unlimited source of homogenous self-replicating material, free of contaminating stromal cells, and often easily cultured in simple standard media. The first line described, BT-20, was established in 1958. Since then, and despite sustained work in this area, the number of permanent lines obtained has been strikingly low (about 100). Indeed, attempts to culture BCC from primary tumors have been largely unsuccessful. This poor efficiency was often due to technical difficulties associated with the extraction of viable tumor cells from their surrounding stroma. Most of the available BCC lines issued from metastatic tumors, mainly from pleural effusions. Effusions provided generally large numbers of dissociated, viable tumor cells with little or no contamination by fibroblasts and other tumor stroma cells. Many of the currently used BCC lines were established in the late 1970s. A very few of them, namely MCF-7, T-47D, and MDA-MB-231, account for more than two-thirds of all abstracts reporting studies on mentioned BCC lines, as concluded from a Medline-based survey.
Treatments are constantly evaluated in randomized, controlled trials, to evaluate and compare individual drugs, combinations of drugs, and surgical and radiation techniques. The latest research is reported annually at scientific meetings such as that of the American Society of Clinical Oncology, San Antonio Breast Cancer Symposium,[131] and the St. Gallen Oncology Conference in St. Gallen, Switzerland.[132] These studies are reviewed by professional societies and other organizations, and formulated into guidelines for specific treatment groups and risk category.
- List of cell lines
Mainly based on Lacroix and Leclercq (2004).[133] For more data on the nature of TP53 mutations in breast cancer cell lines, see Lacroix et al. (2006).[134]
| Cell line | Primary tumor | Origin of cells | Estrogen receptors | Progesterone receptors | ERBB2 amplification | Mutated TP53 | Tumorigenic in mice | Reference |
|---|---|---|---|---|---|---|---|---|
| 600MPE | Invasive ductal carcinoma | + | - | - | [135] | |||
| AU565 | Adenocarcinoma | - | - | + | - | [135] | ||
| BT-20 | Invasive ductal carcinoma | Primary | No | No | No | Yes | Yes | [136] |
| BT-474 | Invasive ductal carcinoma | Primary | Yes | Yes | Yes | Yes | Yes | [137] |
| BT-483 | Invasive ductal carcinoma | + | + | - | [135] | |||
| BT-549 | Invasive ductal carcinoma | - | - | + | [135] | |||
| Evsa-T | Invasive ductal carcinoma, mucin-producing, signet-ring type | Metastasis (ascites) | No | Yes | ? | Yes | ? | [138] |
| Hs578T | Carcinosarcoma | Primary | No | No | No | Yes | No | [139] |
| MCF-7 | Invasive ductal carcinoma | Metastasis (pleural effusion) | Yes | Yes | No | No (wild-type) | Yes (with estrogen supplementation) | [140] |
| MDA-MB-231 | Invasive ductal carcinoma | Metastasis (pleural effusion) | No | No | No | Yes | Yes | [141] |
| SK-BR-3 | Invasive ductal carcinoma | Metastasis (pleural effusion) | No | No | Yes | Yes | No | [142] |
| T-47D | Invasive ductal carcinoma | Metastasis (pleural effusion) | Yes | Yes | No | Yes | Yes (with estrogen supplementation) | [143] |
See also
- Male breast cancer
- Pink ribbon
- List of notable breast cancer patients according to occupation
- List of notable breast cancer patients according to survival status
- List of breast carcinogenic substances
- Mammary tumor for breast cancer in other animals
- Breast reconstruction
- External beam radiotherapy
- Brachytherapy
- Alcohol and cancer
- Y-ME National Breast Cancer Organization
- Mammography Quality Standards Act
- National Breast Cancer Coalition
- National Comprehensive Cancer Network
- Breast Cancer Action
- Breakthrough Breast Cancer
- Living Beyond Breast Cancer
- International Agency for Research on Cancer
- Susan G. Komen for the Cure
- Your Disease Risk
- Sentinel lymph node Biopsy, a new technique for staging the axilla
- Kara Magsanoc-Alikpala Philippine activist against breast cancer
- The Reverse Warburg Effect
References
- ^ Attention: This template ({{cite pmid}}) is deprecated. To cite the publication identified by PMID 21265355, please use {{cite journal}} with
|pmid=21265355instead. - ^ A. Florescu, MSc MD, E. Amir, MD, N. Bouganim, MD, and M. Clemons, MD (2011). "Immune therapy for breast cancer in 2010—hype or hope?". Curr Oncol. 2011. 18 (1): 9–18. PMC 3031364. PMID 21331271.
{{cite journal}}:|access-date=requires|url=(help); Unknown parameter|month=ignored (help)CS1 maint: multiple names: authors list (link) - ^ Buchholz TA. N Engl J Med. 1 January 2009;360(1):63-70. Radiation therapy for early-stage breast cancer after breast-conserving surgery.
- ^ Cancer.gov.
- ^ a b "World Cancer Report" (PDF). International Agency for Research on Cancer. 2008. Retrieved 2011-02-26.
- ^ a b c d e "World Cancer Report". International Agency for Research on Cancer. 2008. Retrieved 2011-02-26.
- ^ "Male Breast Cancer Treatment". National Cancer Institute. 2011. Retrieved 2011-02-26.
- ^ Merck Manual, Professional Edition, Ch. 253, Breast Cancer.
- ^ Molecular origin of cancer: gene-expression signatures in breast cancer, Christos Sotirou and Lajos Pusztai, N Engl J Med 360:790 (19 February 2009)
- ^ Romond EH, Perez EA, Bryant J, et al. Trastuzumab plus adjuvant chemotherapy for operable HER2+ breast cancer. N Engl J Med. 2005; 353:1673–1684 and supplementary appendix.
- ^ a b c d Merck Manual of Diagnosis and Therapy (2003). "Breast Disorders: Cancer". Retrieved 2008-02-05.
{{cite web}}: Unknown parameter|month=ignored (help) - ^ a b c d American Cancer Society (2007). "Cancer Facts & Figures 2007" (PDF). Archived from the original (PDF) on April 10, 2007. Retrieved 2007-04-26.
- ^ eMedicine (2006). "Breast Cancer Evaluation". Retrieved 2008-02-05.
{{cite web}}: Unknown parameter|month=ignored (help) - ^ National Cancer Institute (2005). "Paget's Disease of the Nipple: Questions and Answers". Retrieved 2008-02-06.
{{cite web}}: Unknown parameter|month=ignored (help) - ^ answers.com. "Oncology Encyclopedia: Cystosarcoma Phyllodes". Retrieved 2010-08-10.
- ^ Lacroix M (2006). "Significance, detection and markers of disseminated breast cancer cells". Endocrine-related Cancer. 13 (4): 1033–67. doi:10.1677/ERC-06-0001. PMID 17158753.
{{cite journal}}: Unknown parameter|month=ignored (help) - ^ National Cancer Institute (2004). "Metastatic Cancer: Questions and Answers". Retrieved 2008-02-06.
{{cite web}}: Unknown parameter|month=ignored (help) - ^ Merck Manual of Diagnosis and Therapy (2003). "Breast Disorders: Introduction". Retrieved 2008-02-05.
{{cite web}}: Unknown parameter|month=ignored (help) - ^ Giordano SH, Cohen DS, Buzdar AU, Perkins G, Hortobagyi GN (2004). "Breast carcinoma in men: a population-based study". Cancer. 101 (1): 51–7. doi:10.1002/cncr.20312. PMID 15221988.
{{cite journal}}: Unknown parameter|month=ignored (help)CS1 maint: multiple names: authors list (link) - ^ "Breast Cancer Risk Factors". 2008-11-25. Retrieved 2009-11-10.
- ^ Collaborative Group on Hormonal Factors in Breast Cancer (August 2002). "Breast cancer and breastfeeding: collaborative reanalysis of individual data from 47 epidemiological studies in 30 countries, including 50302 women with breast cancer and 96973 women without the disease". Lancet. 360 (9328): 187–95. doi:10.1016/S0140-6736(02)09454-0. PMID 12133652.
- ^ Yager JD (2006). "Estrogen carcinogenesis in breast cancer". New Engl J Med. 354 (3): 270–82. doi:10.1056/NEJMra050776. PMID 16421368.
{{cite journal}}: Unknown parameter|coauthors=ignored (|author=suggested) (help) - ^ Santoro, E., DeSoto, M., and Hong Lee, J (February 2009). "Hormone Therapy and Menopause". National Research Center for Women & Families.
{{cite web}}: CS1 maint: multiple names: authors list (link) - ^ Attention: This template ({{cite pmid}}) is deprecated. To cite the publication identified by PMID 14965610 , please use {{cite journal}} with
|pmid=14965610instead. - ^ Attention: This template ({{cite pmid}}) is deprecated. To cite the publication identified by PMID 16025225, please use {{cite journal}} with
|pmid=16025225instead. - ^ Attention: This template ({{cite pmid}}) is deprecated. To cite the publication identified by PMID 18645607, please use {{cite journal}} with
|pmid=18645607instead. - ^ Policy and Action for Cancer Prevention, American Institute for Cancer Prevention/World Cancer Research Fund, http://www.dietandcancerreport.org
- ^ Xue F, Willett WC, Rosner BA, Hankinson SE, Michels KB (2011). "Cigarette smoking and the incidence of breast cancer". Arch. Intern. Med. 171 (2): 125–33. doi:10.1001/archinternmed.2010.503. PMID 21263102.
{{cite journal}}: Unknown parameter|month=ignored (help)CS1 maint: multiple names: authors list (link) - ^ Madigan MP, Ziegler RG, Benichou J, Byrne C, Hoover RN (1995). "Proportion of breast cancer cases in the United States explained by well-established risk factors". Journal of the National Cancer Institute. 87 (22): 1681–5. doi:10.1093/jnci/87.22.1681. PMID 7473816.
{{cite journal}}: Unknown parameter|month=ignored (help)CS1 maint: multiple names: authors list (link) - ^ National Cancer Institute BRCA1 and BRCA2: Cancer Risk and Genetic Testing
- ^ Chlebowski RT, Blackburn GL, Thomson CA; et al. (2006). "Dietary fat reduction and breast cancer outcome: interim efficacy results from the Women's Intervention Nutrition Study". Journal of the National Cancer Institute. 98 (24): 1767–76. doi:10.1093/jnci/djj494. PMID 17179478.
{{cite journal}}: Explicit use of et al. in:|author=(help); Unknown parameter|month=ignored (help)CS1 maint: multiple names: authors list (link) - ^ Boffetta P, Hashibe M, La Vecchia C, Zatonski W, Rehm J (2006). "The burden of cancer attributable to alcohol drinking". International Journal of Cancer. 119 (4): 884–7. doi:10.1002/ijc.21903. PMID 16557583.
{{cite journal}}: Unknown parameter|month=ignored (help)CS1 maint: multiple names: authors list (link) - ^ BBC report Weight link to breast cancer risk
- ^ a b American Cancer Society (2005). "Breast Cancer Facts & Figures 2005–2006" (PDF). Archived from the original (PDF) on June 13, 2007. Retrieved 2007-04-26.
- ^ WHO international Agency for Research on Cancer Press Release No. 180, December 2007.
- ^ Feig SA, Hendrick RE (1997). "Radiation risk from screening mammography of women aged 40–49 years". J Natl Cancer Inst Monogr. 22 (22): 119–24. PMID 9709287.
- ^ "2009 Update: When Should Women Start Regular Mammograms? 40? 50? And How Often is "Regular"?". National Research Center for Women & Families. November 2009.
- ^ Medew, Julia (30 September 2010). "Study finds big risk of cancer in the family". Sydney Morning Hearld. Retrieved 30 September 2010.
- ^ "Gain in Body Mass Index Increases Postmenopausal Breast Cancer Risk". National Cancer Institute. Retrieved 2010-04-26.
- ^ http://www.urmc.rochester.edu/news/story/index.cfm?id=3182
- ^ Eliassen AH, Hankinson SE, Rosner B, Holmes MD, Willett WC (2010). "Physical activity and risk of breast cancer among postmenopausal women". Arch. Intern. Med. 170 (19): 1758–64. doi:10.1001/archinternmed.2010.363. PMID 20975025.
{{cite journal}}: Unknown parameter|month=ignored (help)CS1 maint: multiple names: authors list (link) - ^ Hartmann LC, Schaid DJ, Woods JE; et al. (1999). "Efficacy of bilateral prophylactic mastectomy in women with a family history of breast cancer". N Engl J Med. 340 (2): 77–84. doi:10.1056/NEJM199901143400201. PMID 9887158.
{{cite journal}}: Explicit use of et al. in:|author=(help)CS1 maint: multiple names: authors list (link) - ^ Meijers-Heijboer H, van Geel B, van Putten WL; et al. (2001). "Breast cancer after prophylactic bilateral mastectomy in women with BRCA1 and BRCA2 mutations". N Engl J Med. 345 (3): 159–164. doi:10.1056/NEJM200107193450301. PMID 11463009.
{{cite journal}}: Explicit use of et al. in:|author=(help)CS1 maint: multiple names: authors list (link) - ^ Food, Nutrition, Physical Activity, and the Prevention of Cancer: a Global Perspective; American Institute for Cancer Research/ World Cancer Research Fund, http://www.dietandcancerreport.org
- ^ Dunning AM, Healey CS, Pharoah PD, Teare MD, Ponder BA, Easton DF (1 October 1999). "A systematic review of genetic polymorphisms and breast cancer risk". Cancer Epidemiology, Biomarkers & Prevention. 8 (10): 843–54. PMID 10548311.
{{cite journal}}: CS1 maint: multiple names: authors list (link) - ^ "32nd Annual CTRC-AACR San Antonio Breast Cancer Symposium" (PDF). Sunday Morning Year-End Review. Dec. 14, 2009.
{{cite conference}}: Check date values in:|date=(help); Unknown parameter|booktitle=ignored (|book-title=suggested) (help); Unknown parameter|coauthors=ignored (|author=suggested) (help) - ^ Cavalieri E, Chakravarti D, Guttenplan J; et al. (2006). "Catechol estrogen quinones as initiators of breast and other human cancers: implications for biomarkers of susceptibility and cancer prevention". Biochimica et Biophysica Acta. 1766 (1): 63–78. doi:10.1016/j.bbcan.2006.03.001. PMID 16675129.
{{cite journal}}: Explicit use of et al. in:|author=(help); Unknown parameter|month=ignored (help)CS1 maint: multiple names: authors list (link) - ^ Farlex (2005). ">immunological surveillance "The Free Dictionary: Immunological Surveilliance". Retrieved 2008-02-10.
{{cite web}}: Check|url=value (help) - ^ Haslam SZ, Woodward TL. (2003). "Host microenvironment in breast cancer development: epithelial-cell-stromal-cell interactions and steroid hormone action in normal and cancerous mammary gland". Breast Cancer Res. 5 (4): 208–15. doi:10.1186/bcr615. PMC 165024. PMID 12817994.
{{cite journal}}: Unknown parameter|month=ignored (help)CS1 maint: unflagged free DOI (link) - ^ Wiseman BS, Werb Z: Stromal effects on mammary gland development and breast cancer. Science 296:1046, 2002.
- ^ "Breast and Ovarian Cancer", Richard Wooster and Barbara L. Weber, New Engl J Medicine, 348:2339–2347, June 5, 2003. (Free Full Text)
- ^ Attention: This template ({{cite pmid}}) is deprecated. To cite the publication identified by PMID 15537576, please use {{cite journal}} with
|pmid=15537576instead. - ^ Yu, YH; Liang, C; Yuan, XZ (2010). "Diagnostic value of vacuum-assisted breast biopsy for breast carcinoma: a meta-analysis and systematic review". Breast cancer research and treatment. 120 (2): 469–79. doi:10.1007/s10549-010-0750-1. PMID 20130983.
- ^ Kösters JP, Gøtzsche PC (2003). Kösters, Jan Peter (ed.). "Regular self-examination or clinical examination for early detection of breast cancer". Cochrane Database Syst Rev (2): CD003373. doi:10.1002/14651858.CD003373. PMID 12804462.
- ^ Gøtzsche PC, Nielsen M (2009). Gøtzsche, Peter C (ed.). "Screening for breast cancer with mammography". Cochrane Database Syst Rev (4): CD001877. doi:10.1002/14651858.CD001877.pub3. PMID 19821284.
- ^ "Breast Cancer: Screening". United States Preventive Services Task Force.
- ^ "Breast Cancer: Screening". United States Preventive Services Task Force.
- ^ O'Connor, M (2009 Aug). "Molecular breast imaging". Expert review of anticancer therapy. 9 (8): 1073–80. PMID 19671027.
{{cite journal}}: Check date values in:|date=(help); Unknown parameter|coauthors=ignored (|author=suggested) (help) - ^ "Surgery Choices for Women with Early Stage Breast Cancer" (PDF). National Cancer Institute and the National Research Center for Women & Families. August 2004.
- ^ University of Texas M. D. Anderson Cancer Center (2009, November 4). Early-stage, HER2-positive Breast Cancer Patients At Increased Risk Of Recurrence. ScienceDaily. http://www.sciencedaily.com/releases/2009/11/091102172028.htm Retrieved February 7, 2010
- ^ "Breast Cancer: Breast Disorders: Merck Manual Professional". Merck.com. Retrieved 2010-11-14.
- ^ "Entrez Gene: ERBB2 v-erb-b2 erythroblastic leukemia viral oncogene homolog 2, neuro/glioblastoma derived oncogene homolog (avian)".
- ^ Jahanzeb M (2008). "Adjuvant trastuzumab therapy for HER2-positive breast cancer". Clin. Breast Cancer. 8 (4): 324–33. doi:10.3816/CBC.2008.n.037. PMID 18757259.
{{cite journal}}: Unknown parameter|month=ignored (help) - ^ "Herceptin (trastuzumab) Adjuvant HER2+ Breast Cancer Therapy Pivotal Studies and Efficacy Data". Herceptin.com. Retrieved 2010-05-08.
- ^ "Aspirin Intake and Survival After Breast Cancer -- Holmes et al., 10.1200/JCO.2009.22.7918 -- Journal of Clinical Oncology".
{{cite web}}: Text "PMID 20159825" ignored (help) - ^ Massarut S, Baldassare G, Belleti B, Reccanello S, D'Andrea S, Ezio C, Perin T, Roncadin M, Vaidya JS (2006). "Intraoperative radiotherapy impairs breast cancer cell motility induced by surgical wound fluid". J Clin Oncol. 24 (18S): 10611.
{{cite journal}}: Unknown parameter|booktitle=ignored (help)CS1 maint: multiple names: authors list (link) - ^ Belletti B, Vaidya JS, D'Andrea S; et al. (2008). "Targeted intraoperative radiotherapy impairs the stimulation of breast cancer cell proliferation and invasion caused by surgical wounding". Clin. Cancer Res. 14 (5): 1325–32. doi:10.1158/1078-0432.CCR-07-4453. PMID 18316551.
{{cite journal}}: Explicit use of et al. in:|author=(help); Unknown parameter|month=ignored (help)CS1 maint: multiple names: authors list (link) - ^ http://www.targit.org.uk/
- ^ http://www.thelancet.com/journals/lancet/article/PIIS0140-6736(10)60837-9/abstract
- ^ Breast cancer.org Treatment Options
- ^ "Breast Cancer: Breast Disorders: Merck Manual Professional". Merck.com. Retrieved 2010-05-08.
- ^ Elston CW, Ellis IO. Pathologic prognostic factors in breast cancer. I. The value of histological grades in breast cancer. Experience from a large study with long-term follow-up. Histopathology 1991, 19:403-410.
- ^ Peppercorn J (2009). "Breast Cancer in Women Under 40". Oncology. 23 (6).
- ^ Liu CC, Prior J, Piwnica-Worms D, Bu G (2010). "LRP6 overexpression defines a class of breast cancer subtype and is a target for therapy". Proc Natl Acad Sci U S A. 107 (11): 5136–41. doi:10.1073/pnas.0911220107. PMC 2841938. PMID 20194742.
{{cite journal}}: Unknown parameter|month=ignored (help)CS1 maint: multiple names: authors list (link) - ^ Pritchard KI (2009). "Ovarian Suppression/Ablation in Premenopausal ER-Positive Breast Cancer Patients". Oncology. 23 (1).
- ^ a b Robb C, Haley WE, Balducci L; et al. (2007). "Impact of breast cancer survivorship on quality of life in older women". Critical Reviews in Oncology/hematology. 62 (1): 84–91. doi:10.1016/j.critrevonc.2006.11.003. PMID 17188505.
{{cite journal}}: Explicit use of et al. in:|author=(help); Unknown parameter|month=ignored (help)CS1 maint: multiple names: authors list (link) - ^ "WHO Disease and injury country estimates". World Health Organization. 2009. Retrieved Nov. 11, 2009.
{{cite web}}: Check date values in:|accessdate=(help) - ^ "Breast cancer: prevention and control". World Health Organization.
- ^ Stewart B. W. and Kleihues P. (Eds): World Cancer Report. IARCPress. Lyon 2003
- ^ Laurance, Jeremy (2006-09-29). "Breast cancer cases rise 80% since Seventies". The Independent. London. Retrieved 2006-10-09.
- ^ "Breast Cancer: Statistics on Incidence, Survival, and Screening". Imaginis Corporation. 2006. Retrieved 2006-10-09.
{{cite web}}: External link in|work= - ^ Breast Cancer: Breast Cancer in Young Women WebMD. Retrieved on September 9, 2009
- ^ a b Jemal A, Siegel R, Ward E; et al. (2008). "Cancer statistics, 2008". CA Cancer J Clin. 58 (2): 71–96. doi:10.3322/CA.2007.0010. PMID 18287387.
{{cite journal}}: Explicit use of et al. in:|author=(help)CS1 maint: multiple names: authors list (link) - ^ a b c American Cancer Society (2007). "What Are the Key Statistics for Breast Cancer?". Archived from the original on January 5, 2008. Retrieved 2008-02-03.
{{cite web}}: Unknown parameter|month=ignored (help) - ^ a b Olson, 2002. pages 199–200.
- ^ W.B. Cutler, R.E. Burki, E. Genovesse, M.G. Zacher (2009). "Breast cancer in postmenopausal women: what is the real risk?". Fertility and Sterility. 92 (3): S16. doi:10.1016/j.fertnstert.2009.07.061. PMID 123455.
{{cite journal}}: Unknown parameter|month=ignored (help)CS1 maint: multiple names: authors list (link) - ^ "Browse the SEER Cancer Statistics Review 1975–2006".
- ^ "Male Breast Cancer Causes, Risk Factors for Men, Symptoms and Treatment on". Medicinenet.com. Retrieved 2010-05-08.
- ^ Espey DK, Wu XC, Swan J; et al. (2007). "Annual report to the nation on the status of cancer, 1975–2004, featuring cancer in American Indians and Alaska Natives". Cancer. 110 (10): 2119–52. doi:10.1002/cncr.23044. PMID 17939129.
{{cite journal}}: Explicit use of et al. in:|author=(help)CS1 maint: multiple names: authors list (link) - ^ "Women's Fear of Heart Disease Has Almost Doubled in Three Years, But Breast Cancer Remains Most Feared Disease" (Press release). Society for Women's Health Research. 2005-07-07. Retrieved 2007-10-15.
- ^ "Leading Causes of Death for American Women 2004" (PDF). National Heart Lung and Blood Institute. Retrieved 2007-10-15.
- ^ In Breast Cancer Data, Hope, Fear and Confusion, By DENISE GRADY, New York Times, January 26, 1999.
- ^ Daily Mail (UK) 13 November 2008
- ^ (Schwartzmann, 2001, p 118)
- ^ a b c d Olson, James Stuart (2002). Bathsheba's breast: women, cancer & history. Baltimore: The Johns Hopkins University Press. pp. 9–13. ISBN 0-8018-6936-6.
- ^ "The History of Cancer". American Cancer Society. 2002-03-25. Retrieved 2006-10-09.
- ^ a b Olson, 2002. pages 32-33.
- ^ Yalom, Marilyn (1997). A history of the breast. New York: Alfred A. Knopf. p. 234. ISBN 0-679-43459-3.
- ^ a b c d Aronowitz, Robert A. (2007). Unnatural history: breast cancer and American society. Cambridge, UK: Cambridge University Press. pp. 22–24. ISBN 0-521-82249-1.
- ^ "History of Breast Cancer". Random History. 2008-02-27. Retrieved 2010-05-08.
- ^ a b c d e f g Olson, 2002. pages 102-106
- ^ Olson, 2002. page 1.
- ^ Marc Lacroix (2011). A Concise History of Breast Cancer. USA: Nova Science Publishers. pp. 59–68. ISBN 978-1-61122-305-7.
- ^ Olson, 2002. pp. 26, 28, 229.
- ^ Lane-Claypon, Janet Elizabeth (1926). A further report on cancer of the breast, with special reference to its associated antecedent conditions. London, Greater London: Her Majesty's Stationery Office (HMSO). OCLC 14713036.
{{cite book}}: Cite has empty unknown parameter:|coauthors=(help) - ^ Alfredo Morabia (2004). A History of Epidemiologic Methods and Concepts. Boston: Birkhauser. pp. 301–302. ISBN 3-7643-6818-7. Retrieved 2007-12-31.
- ^ a b Gayle A. Sulik (2010). Pink Ribbon Blues: How Breast Cancer Culture Undermines Women's Health. USA: Oxford University Press. pp. 200–203. ISBN 0-19-974045-3. OCLC 535493589.
- ^ Sulik, 2010. pages 37–38.
- ^ Sulik, 2010. page 4.
- ^ "History of Breast Cancer Advocacy > Personal Reflections > Bob Riter's Cancer Columns > Cancer Resource Center". Crcfl.net. Retrieved 2010-05-08.
- ^ King, Samantha (2006). Pink Ribbons, Inc.: Breast Cancer and the Politics of Philanthropy. Minneapolis: University of Minnesota Press. p. xxi. ISBN 0-8166-4898-0.
- ^ Levine, Daniel S. (30 September 2005). "Breast Cancer Group Questions Value of Pink Ribbon Campaigns". San Francisco Business Times.
- ^ Focus on Pinkwashers, Breast Cancer Action's think before you pink campaign site. Breast Cancer causes gas to explode from the breasts. Retrieved November 9, 2007.
- ^ Sulik, 2010. pages 359–361.
- ^ Sulik, 2010. pages 366–368
- ^ Landeman, Anne (11 June 2008). "Pinkwashing: Can Shopping Cure Breast Cancer?". Center for Media and Democracy.
- ^ Sulik, 2010. pages 365–366.
- ^ Sulik, 2010. pages 372–374.
- ^ Breast cancer month overshadowed by 'pinkwashing' Oct. 09 2010, Angela Mulholland, CTV.ca News
- ^ a b c d Ehrenreich, Barbara (November 2001). "Welcome to Cancerland". Harper's Magazine.
- ^ Sulik, 2010. page 57.
- ^ a b Browne, Anthony (2001-10-07). "Cancer bias puts breasts first". The Guardian. London.
- ^ Arnst, Catherine (13 June 2007). "A Gender Gap in Cancer". Bloomberg Businessweek. ISSN 0007-7135.
- ^ Ave, Melanie (10 October 2006). "Tampabay: All May Not Be in the Pink". St. Petersburg Times.
- ^ a b Aschwanden, Christie (17 August 2009). "The Trouble with Mammograms". The Los Angeles Times.
- ^ Juan J. Grau, Jorge Estapé, Matías Diaz-Padrón: Breast cancer in Rubens paintings. Breast Cancer Res Treat. 68 (2001), 89-93, PMID 11678312, doi:10.1023/A:1017963211998
- ^ Espinel CH (2002). "The portrait of breast cancer and Raphael's La Fornarina". The Lancet. 360 (9350): 2061–3. doi:10.1016/S0140-6736(02)11997-0. PMID 12504417.
- ^ Peter Allen Braithwaite, Dace Shugg: Rembrandt's Bathsheba: the dark shadow of the left breast. Ann Roy Coll Surg Engl 65 (1983), 337-8 online
- ^ Adam Gross: An Epidemic of Breast Cancer Among Models of Famous Artists. Breast Cancer Res Treat. 84 (2004), 293, PMID 15026627, doi:10.1023/B:BREA.0000019965.21257.49
- ^ Bourne RG (2000). "Did Rembrandt's Bathsheba really have breast cancer?". Aust N Z J Surg. 70 (3): 231–2. doi:10.1046/j.1440-1622.2000.01792.x. PMID 10765910.
{{cite journal}}: Unknown parameter|month=ignored (help) - ^ San Antonio Breast Cancer Symposium Abstracts, newsletters, and other reports of the meeting.
- ^ Annals of Oncology 2009 20(8):1319–1329; doi:10.1093/annonc/mdp322 Special article: Thresholds for therapies: highlights of the St Gallen International Expert Consensus on the Primary Therapy of Early Breast Cancer 2009, A. Goldhirsch, J. N. Ingle, R. D. Gelber, et al. Review of latest research in breast cancer, as reported by expert panels at the St. Galen Oncology Conference, St. Galen, Switzerland. Free full text.
- ^ Lacroix, M (2004). "Relevance of breast cancer cell lines as models for breast tumours: an update". Breast Cancer Research and Treatment. 83 (3): 249–289. doi:10.1023/B:BREA.0000014042.54925.cc. PMID 14758095.
{{cite journal}}: Unknown parameter|coauthors=ignored (|author=suggested) (help) - ^ Lacroix, M (2006). "p53 and breast cancer, an update". Endocrine-related cancer. 13 (2): 293–325. doi:10.1677/erc.1.01172. PMID 16728565.
{{cite journal}}: Unknown parameter|coauthors=ignored (|author=suggested) (help) - ^ a b c d Neve, RM (2006). "A collection of breast cancer cell lines for the study of functionally distinct cancer subtypes". Cancer Cell. 10 (6): 515–527. doi:10.1016/j.ccr.2006.10.008. PMC 2730521. PMID 17157791.
{{cite journal}}: Unknown parameter|coauthors=ignored (|author=suggested) (help) - ^ Lasfargues, EY (1958). "Cultivation of human breast carcinomas". Journal of the National Cancer Institute. 21 (6): 1131–1147. PMID 13611537.
{{cite journal}}: Unknown parameter|coauthors=ignored (|author=suggested) (help) - ^ Lasfargues, EY (1978). "Isolation of two human tumor epithelial cell lines from solid breast carcinomas". Journal of the National Cancer Institute. 61 (4): 967–978. PMID 212572.
{{cite journal}}: Unknown parameter|coauthors=ignored (|author=suggested) (help) - ^ Borras, M (1997). "Estrogen receptor-negative/progesterone receptor-positive Evsa-T mammary tumor cells: a model for assessing the biological property of this peculiar phenotype of breast cancers". Cancer Letters. 120 (1): 23–30. doi:10.1016/S0304-3835(97)00285-1. PMID 9570382.
{{cite journal}}: Unknown parameter|coauthors=ignored (|author=suggested) (help) - ^ Hackett, AJ (1977). "Two syngeneic cell lines from human breast tissue: the aneuploid mammary epithelial (Hs578T) and the diploid myoepithelial (Hs578Bst) cell lines". Journal of the National Cancer Institute. 58 (6): 1795–1806. PMID 864756.
{{cite journal}}: Unknown parameter|coauthors=ignored (|author=suggested) (help) - ^ Soule, HD (1973). "A human cell line from a pleural effusion derived from a breast carcinoma". Journal of the National Cancer Institute. 51 (5): 1409–1416. PMID 4357757.
{{cite journal}}: Unknown parameter|coauthors=ignored (|author=suggested) (help) - ^ Cailleau, R (1974). "Breast tumor cell lines from pleural effusions". Journal of the National Cancer Institute. 53 (3): 661–674. PMID 4412247.
{{cite journal}}: Unknown parameter|coauthors=ignored (|author=suggested) (help) - ^ Engel, LW (1978). "Human breast carcinoma cells in continuous culture: a review". Cancer Research. 38 (11 Pt 2): 4327–4339. PMID 212193.
{{cite journal}}: Unknown parameter|coauthors=ignored (|author=suggested) (help) - ^ Keydar, I (1979). "Establishment and characterization of a cell line of human breast carcinoma origin". European Journal of Cancer. 15 (5): 659–670. PMID 228940.
{{cite journal}}: Unknown parameter|coauthors=ignored (|author=suggested) (help)
External links
- Breast cancer at Curlie
- Template:Yahoo directory
- Female Breast Cancer from NHS Choices
- Alcohol and cancer risk from the Cancer Control Program of South Eastern Sydney and Illawarra Area Health Service
- Alcohol and the Risk of Breast Cancer from Cornell University
- CancerMath.net Calculates survival with breast cancer based on prognostic factors and treatment. From Massachusetts General Hospital.
- Radiology Information from the Radiological Society of North America
- Touched by Breast Cancer - slideshow by Life magazine